Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Interstitial lung disease (ILD) and small airways disease (SAD) are frequent pulmonary manifestations of primary Sjögren’s disease (SjD). The relation between these two entities and their real prevalence in SjD patients with subjective complaints of respiratory disease are still elusive. Our purpose was to describe the clinical, functional and imaging findings of pulmonary disease in SjD and investigate the association with serologic features and the salivary gland biopsy focus score.
Methods: Consecutive SjD patients with respiratory symptoms and/or asymptomatic patients with abnormal pulmonary function tests, followed up in the Department of Pathophysiology (member of the European Reference Network, ERN), were recruited prospectively, from October 2022 to March 2024. Abnormal PFTs were defined as FVC< 80% and/or FEF25-75< 60% and/or DLCO< 70%. A hundred and one patients with primary SjD comprised the study group. All patients: i) underwent pulmonary and small airways function assessment with spirometry, measurement of DLCO, single breath nitrogen washout, impulse oscillometry, ii) high resolution computed tomography (HRCT) of the lungs evaluated blindly by a specialized radiologist for the presence of ILD and SAD according to international consensus criteria1, and iii) replied to specific questionnaires for dyspnea and cough.
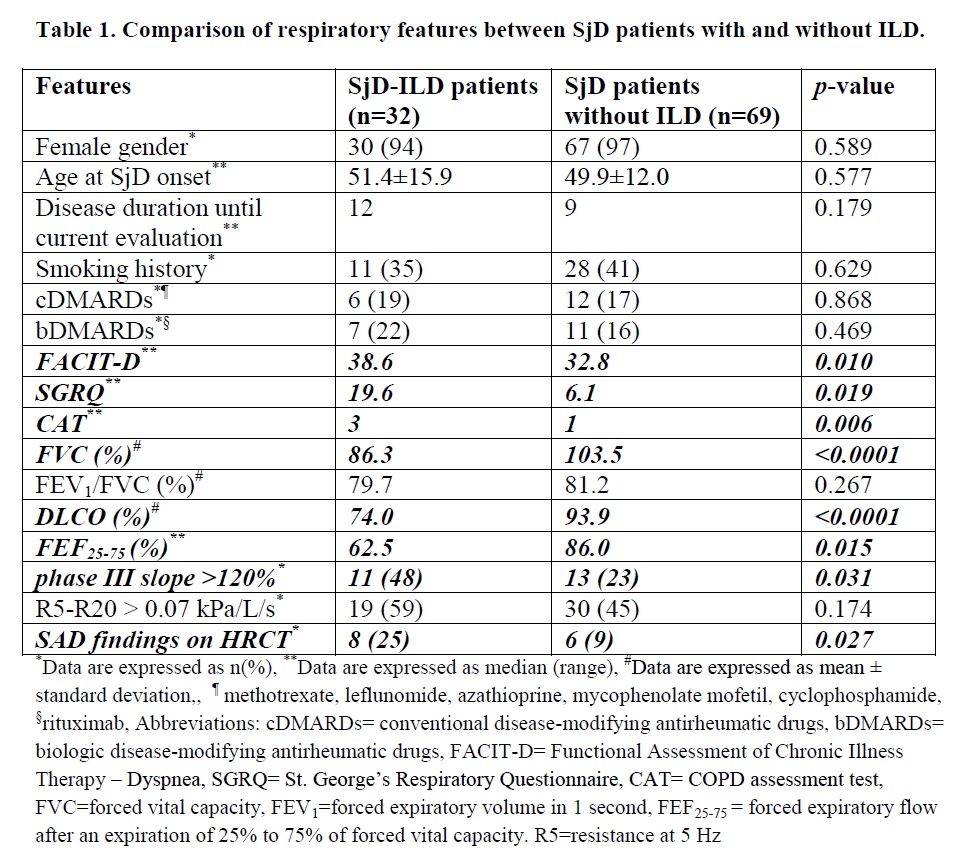
Results: The mean±SD age of the 101 (96% females) patients at SjD onset was 50.7±13.1 years and the median disease duration from SjD onset until current evaluation was 10 years (range: 0-38). Eighty five patients were symptomatic. Thirty two (31.7%) patients had findings of ILD on HRCT. No statistical differences were identified between SjD patients with and without ILD in terms of sex, age at SjD, disease duration, treatment modalities and smoking history (Table 1). SjD-ILD patients presented more frequently with dyspnea and cough assessed by the respiratory questionnaires [FACIT-D (median: 38.6 vs. 32.8, p=0.010), SGRQ (median: 19.6 vs. 6.1, p=0.019), CAT (median: 3 vs. 1, p=0.006)] compared to non ILD-SjD patients. They also had worse small airways function indices [lower FEF25-75 (median: 62.5% vs. 86%, p=0.015), higher R5-R20 (median: 0.100 vs. 0.064 kPa/L/s, p=0.030) and more frequently abnormal phase III slope >120% (48% vs. 23%, p=0.031)] as well as SAD findings on HRCT than non-ILD controls (25% vs. 9%, p=0.027). SjD-ILD patients had more frequently elevated CRP at the time of evaluation (28% vs. 7%, p=0.017), higher disease activity (ESSDAI 4 vs. 2, p=0.003), lymphoma history (33% vs. 10%, p=0.005) and a tendency to develop more frequently anti-Ro52 (80% vs. 61%, p=0.071). Interestingly, at SjD diagnosis SjD-ILD patients had higher focus score on salivary gland biopsy (3.56 vs. 1.50, p=0.002) and lower unstimulated salivary flow (0.60 vs. 1.85 ml/15min, p=0.012).
Conclusion: Interstitial lung disease and small airways disease occur frequently among SjD patients. Interstitial lung disease is associated with worse SAD leading to respiratory symptoms and functional lung impairment, as well as higher focus score at SjD diagnosis and higher disease activity.
References
1. Hansell et al. Radiology (2008) 246:697–722.
To cite this abstract in AMA style:
Panagopoulos P, chatzis L, Chatzinikita E, Malagari K, Vassilakopoulos T, Tzioufas A, Goules A. Prospective Evaluation of Pulmonary Involvement in Patients with Primary Sjögren’s Disease, Using Pulmonary Function Tests and High Resolution Computed Tomography, Reveals High Prevalence of Subclinical Interstitial Lung Disease, Along with Small Airways Disease [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/prospective-evaluation-of-pulmonary-involvement-in-patients-with-primary-sjgrens-disease-using-pulmonary-function-tests-and-high-resolution-computed-tomography-reveals-high-prevalence/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/prospective-evaluation-of-pulmonary-involvement-in-patients-with-primary-sjgrens-disease-using-pulmonary-function-tests-and-high-resolution-computed-tomography-reveals-high-prevalence/