Session Information
Date: Saturday, November 6, 2021
Title: RA – Diagnosis, Manifestations, & Outcomes Poster I: Cardiovascular Pulmonary Disease (0268–0295)
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Rheumatoid arthritis-related lung disease (RA-LD) is a common manifestation of rheumatoid arthritis (RA) and associated with excess mortality. Many studies to date were focused on RA-associated interstitial lung disease (RA-ILD). There are few studies reporting the whole lung manifestations of RA. In this study, we aimed to determine the prevalence of RA-LD and to assess the predictors of mortality in RA-LD patients.
Methods: Patients who attended our rheumatology clinic between January 2010-December 2020 and fulfilled 2010 ACR/EULAR classification criteria for RA were retrospectively evaluated. Among them, patients with abnormal computed tomography of the chest (chest-CT) were scrutinized. RA-LD was defined as the existence of RA-ILD, airway disease (AD), rheumatoid pulmonary nodules (RA-PN) or RA-related pleural effusion (RA-PE). Thoracentesis or lung biopsy results were also used to confirm the existence of RA-LD. The patient data was recorded for each subtype of RA-LD. The date of RA-LD diagnosis was considered the date of the first chest-CT detecting the pathology. To assess the predictors associated with all-cause mortality, logistic regression analysis was performed.
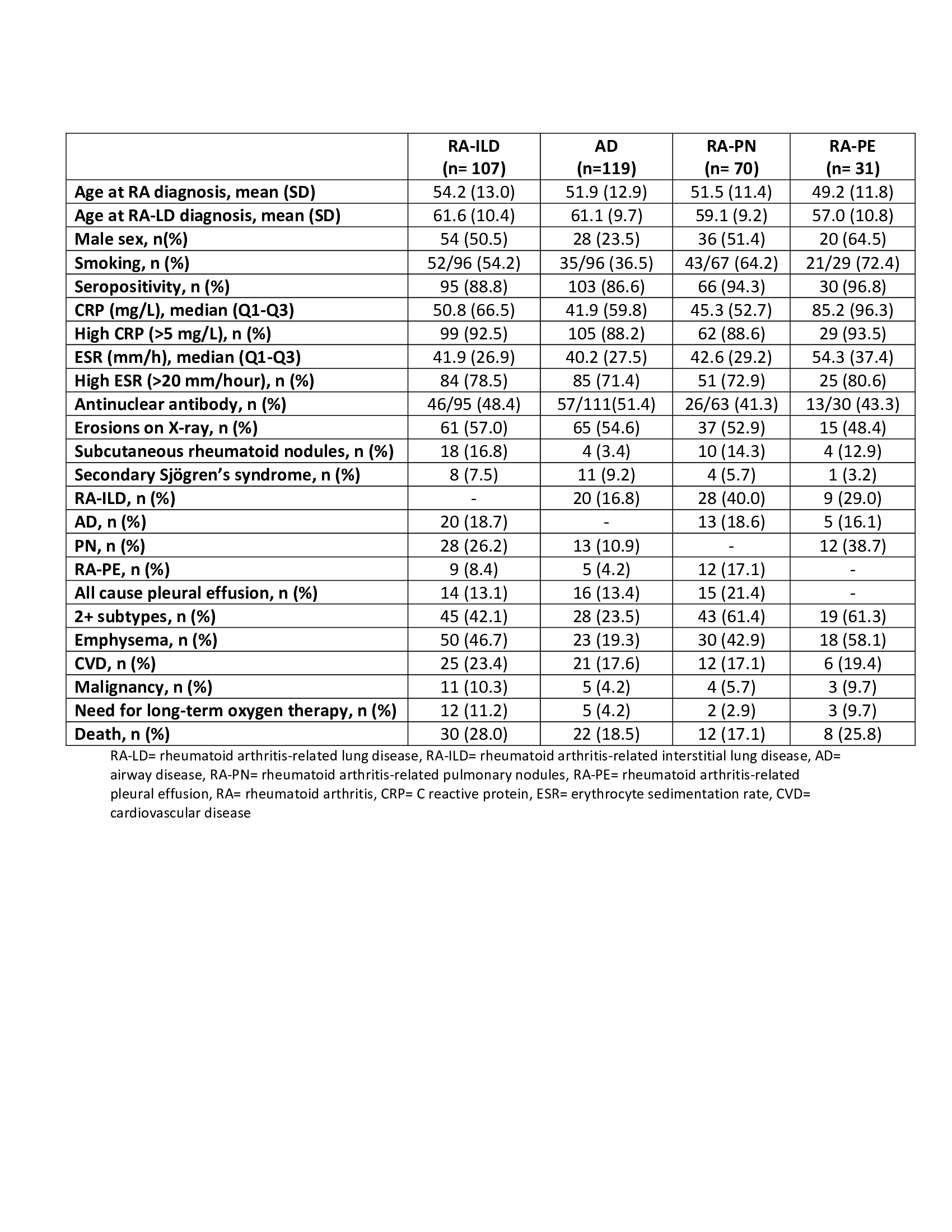
Results: Among 9756 RA patients, 253 (2.6%) patients (38.7% male; mean age at RA and RA-LD diagnoses 52.1 ± 12.4 and 59.9 ± 9.8 years, respectively) had RA-LD. AD was the most common subtype of RA-LD and detected in 119 (47.0%) patients followed by 107 (42.3%) patients with RA-ILD, 70 (27.7%) patients with RA-PN and 31 (12.3%) patients with RA-PE (Figure 1). The characteristics of patients with each subtype are shown in Table 1. Sixty-one (24.1%) patients had 2 or more RA-LD subtypes during their follow-up. After a median of 3.9 years (IQR 5.1), 52 (20.6%) patients died and the 5-year survival rate was 81.8%. In multivariable logistic regression analysis, the existence of RA-ILD, pleural effusion and older age at RA-LD diagnosis were positively associated with higher mortality (odds ratios (OR) were 2.28, 3.30 and 1.04, respectively), whereas methotrexate usage was protective (OR 0.40) (Table 2).
Conclusion: In this single center retrospective study, we showed that the prevalence and mortality of RA-LD was approximately 3% and 20%, respectively. As well as RA-ILD and older age, which are known risk factors, having pleural effusion was also related to mortality. Patients, who received methotrexate, had low mortality rates.


To cite this abstract in AMA style:
Sahin Eroglu D, Colaklar A, Baysal S, Torgutalp M, Baygul A, Sezer S, Aydemir Guloksuz E, Yuksel M, Yayla M, Uslu yurteri E, Uzun C, Ozdemir kumbasar O, Turgay M, Gulay K, Ates A. Prevalence and Predictors of Mortality in Rheumatoid Arthritis-Related Lung Disease: Results from a Single Center Study [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/prevalence-and-predictors-of-mortality-in-rheumatoid-arthritis-related-lung-disease-results-from-a-single-center-study/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/prevalence-and-predictors-of-mortality-in-rheumatoid-arthritis-related-lung-disease-results-from-a-single-center-study/