Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Erosive hand osteoarthritis (HOA) poses challenges due to its aggressive nature and limited epidemiological insights. We aimed to describe the prevalence and joint involvement patterns of erosive and non-erosive HOA.
Methods: Participants aged 50 years or older underwent posteroanterior radiographs of both hands in the Xiangya Osteoarthritis Study, a community-based observational study in China. Erosive HOA was determined using the Verbruggen-Veys erosive or remodeled phase progression score and OARSI atlas. Non-erosive HOA was defined by the Kellgren-Lawrence scale ≥ 2 without erosive features. We estimated the age and sex-specific prevalence of erosive and non-erosive HOA at the person level and subsequently estimated the prevalence at the joint level. We performed Generalized Estimating Equations (Poisson distribution and log link) to calculate the prevalence ratio (PR) to describe the inter-joint relationship of each type of HOA, focusing on symmetry (i.e., same joint in the opposite hand), row (i.e., joints in the same row of the same hand), and ray (i.e., joints in the same ray of the same hand). In the regression models, we adjusted for age, sex, BMI, smoking status, alcohol consumption, education level, and hand injury history.
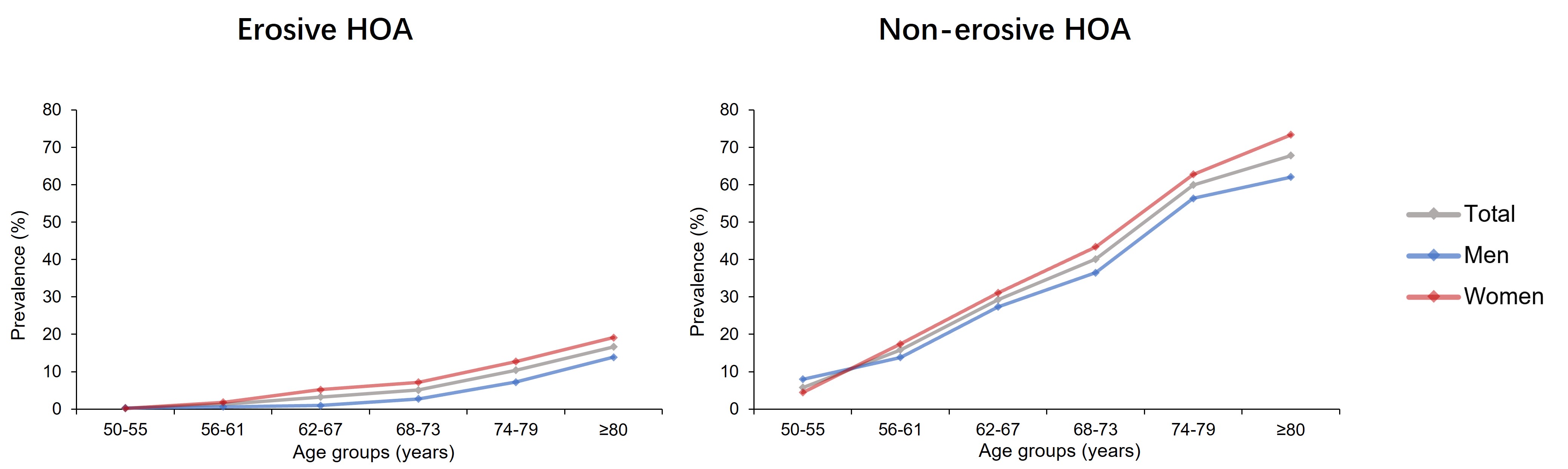
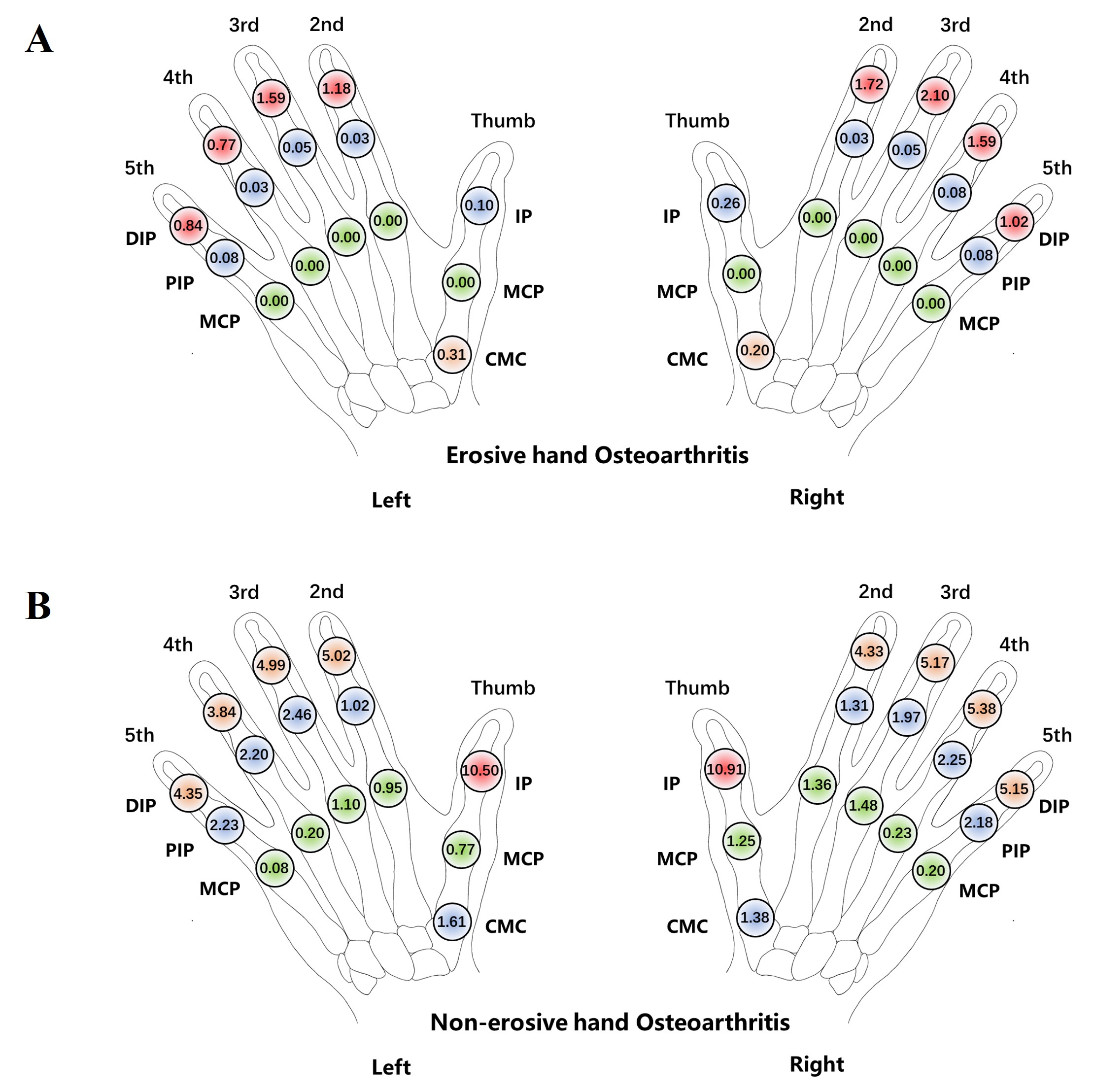
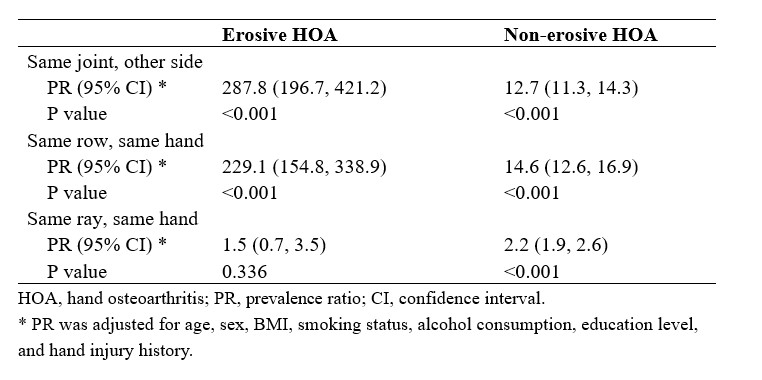
Results: Among the 3,906 participants, the prevalence of erosive and non-erosive HOA was 4.02% and 26.50%, respectively. The prevalence of both erosive and non-erosive HOA increased with age, and was higher in men than in women between the ages 50-55, but was higher in women than in men among those aged 55 years or older (Figure 1). Both erosive and non-erosive HOA often involved multiple joints. However, erosive HOA predominantly affected distal interphalangeal (DIP) joints, with a prevalence ranging from 0.77% to 2.10%, and no case affected the metacarpophalangeal (MCP) joints of the fingers or thumb (Figure 2A). In contrast, non-erosive HOA mainly targeted thumb interphalangeal joints (10%) and could affect the finger and thumb MCP joints (Figure 2B). Erosive HOA displayed significant symmetry (PR = 287.8, 95% confidence interval [CI]: 196.7, 421.2) and clustering by row (PR = 229.1, 95%CI: 154.8, 338.9), but not by ray (PR = 1.5, 95%CI: 0.7, 3.5). Non-erosive HOA also showed symmetry (PR = 12.7, 95%CI: 11.3, 14.3) and clustering both by row (PR = 14.6, 95%CI: 12.6, 16.9) and by ray (PR = 2.2, 95%CI: 1.9, 2.6) (Table 1).
Conclusion: The prevalence of both erosive and non-erosive HOA increased with age and was higher among women than men among those aged 55 years or older. Erosive HOA displayed symmetry and clustering by row but not by ray and did not affect MCP joints. In contrast, non-erosive HOA exhibited symmetry, clustering both by row and by ray, and did involve MCP joints. These findings support the view that erosive and non-erosive HOA are distinct conditions with a different pathophysiology.
To cite this abstract in AMA style:
Ye J, Wang Y, Yang T, Hunter D, Zhang Y, Zhang W, Doherty M, Li J, Li w, Wen Z, Zeng C, Lei G, Wei J. Prevalence and Joint Involvement Patterns of Erosive and Non-erosive Hand Osteoarthritis in the General Population in China [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/prevalence-and-joint-involvement-patterns-of-erosive-and-non-erosive-hand-osteoarthritis-in-the-general-population-in-china/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/prevalence-and-joint-involvement-patterns-of-erosive-and-non-erosive-hand-osteoarthritis-in-the-general-population-in-china/