Session Information
Date: Saturday, November 16, 2024
Title: Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Lung involvement is the most common and severe extra-muscular manifestation of Idiopathic Inflammatory Myopathies (IIM). Early identification of patients at risk for lung transplant or mortality may help improve patient care. This study aimed to evaluate the predictors of lung transplant-free survival in IIM-associated interstitial lung disease (IIM-ILD).
Methods: We retrospectively analyzed clinical data prospectively collected from 1979 to 2014 in a large, observational single-center study. A lead period of 10 years was given for long-term outcomes. We used 2017 EULAR/ACR classification criteria for IIM, with lung involvement defined by radiographic findings on high-resolution computed tomography (HRCT). Collected data included smoking, O2 use, occupational exposure, organ involvement, pulmonary function tests (forced vital capacity [FVC], diffusing capacity for carbon monoxide [DLCO]), HRCT ILD pattern, echocardiogram (ejection fraction and estimated systolic pulmonary artery pressure [ESPAP]), presence of dyspnea, and survival as well as lung transplant data. Univariate analyses for predictors of 5-year transplant-free survival or overall survival were performed using logistic regression.
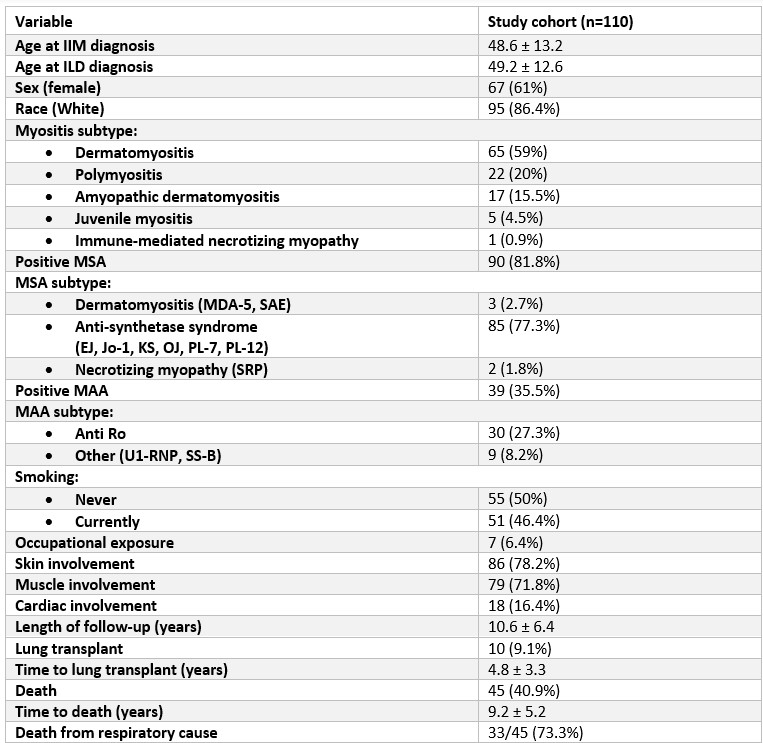
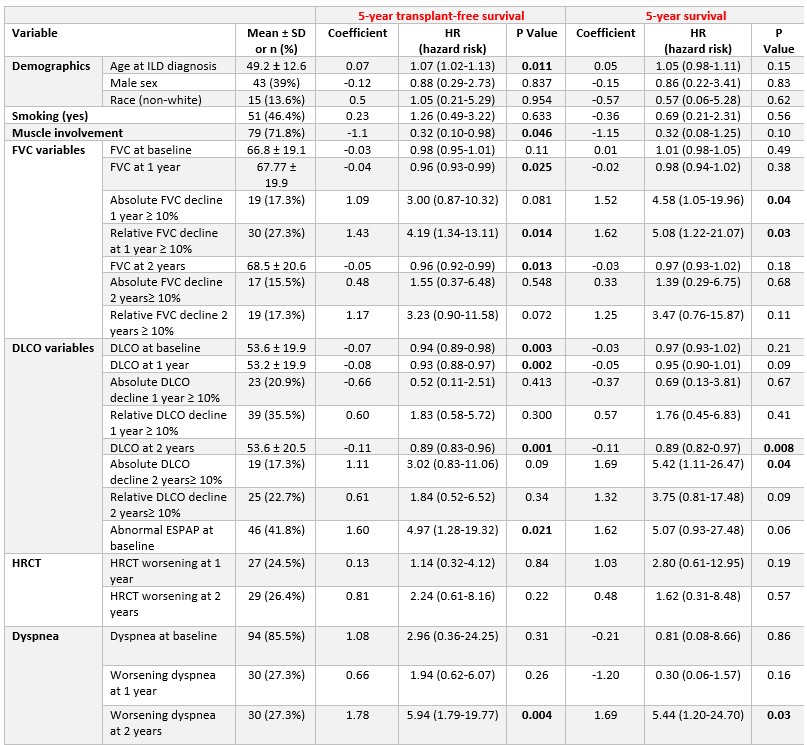
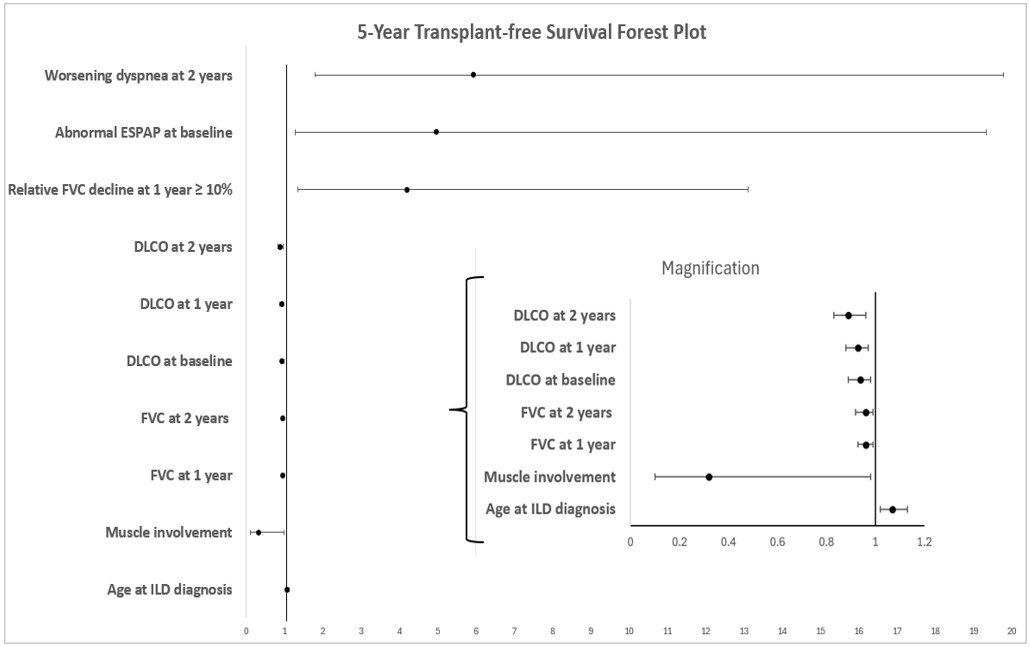
Results: A total of 110 patients with IIM-ILD were evaluated. Patients were predominantly female [67 (61%)] and White [95 (86.4%)], with a mean age 49.2 ± 12.6 years. IIM clinical subtypes included n=65 (59%) dermatomyositis, n=22 (20%) polymyositis, n=17 (15.5%) amyopathic dermatomyositis, n= 5 (4.5%) juvenile myositis, and n=1 (0.9%) immune-mediated necrotizing myopathy. Most patients (77%) had anti-synthetase syndrome. The mean length of follow-up was 10.6 ± 6.4 years. Ten (9.1%) patients underwent lung transplantation after a mean of 4.8 ± 3.3 years, while 45 (41%) died during follow-up after a mean of 9.2 ± 5.2 years [Table 1]. HRCT ILD pattern was NSIP and UIP in 41.8% and 43.6%, respectively. Worsening of HRCT findings occurred in 27 (24.5%) and 29 (26.4%) after 1 and 2 years, respectively. The baseline percent-predicted FVC (%FVC) was 66.8± 19.1, while the baseline %DLCO was 53.6± 19.9. After one year, %FVC declined by an absolute and relative mean of 1.17± 15.3 and 4.7± 28.6, respectively. [Figure 1]. A higher risk of lung transplant or mortality within the first 5 years was associated with increased age (HR 1.07, p=0.01), baseline ESPAP ≥ 30 mmHg (HR 4.97, p=0.02), relative FVC decline at 1 year ≥ 10% (HR=4.2, p=0.01), and worsening dyspnea after 2 years (HR=5.9, p=0.004). Conversely, a lower risk was associated with muscle involvement (HR=0.32, p=0.046), higher baseline DLCO (HR=0.94, P=0.003), and higher FVC at 1 year (HR=0.96, p=0.025). Risk factors for 5-year mortality showed similar results [Table 2].
Conclusion: In patients with IIM-ILD, increased age, pulmonary hypertension, relative decline in FVC at 1 year, and worsening dyspnea at 2 years were significant predictors of mortality or lung transplant within the first 5 years, whereas muscle involvement, higher baseline DLCO, and higher FVC at 1 year were associated with a lower risk of these adverse outcomes. Further research is needed to define ILD progression in myositis patients and improve risk stratification, management, and prognosis.
To cite this abstract in AMA style:
keret s, Silva R, Choudhuri I, Gkiaouraki E, Chandra T, Pongtarakulpanit N, Sriram s, Martinez Laverde s, Ascherman D, Mogahadam S, Oddis C, Aggarwal R. Predictors of Transplant-Free Survival in Idiopathic Inflammatory Myopathies- associated Interstitial Lung Disease [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/predictors-of-transplant-free-survival-in-idiopathic-inflammatory-myopathies-associated-interstitial-lung-disease/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/predictors-of-transplant-free-survival-in-idiopathic-inflammatory-myopathies-associated-interstitial-lung-disease/