Session Information
Date: Monday, November 13, 2023
Title: Abstracts: RA – Diagnosis, Manifestations, & Outcomes II: Comorbidities
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: Long COVID, also known as Post COVID syndrome or postacute sequelae of SARS-CoV-2 infection, refers to the development of persistent or new symptoms lasting for weeks or longer in individuals who have recovered from SARS-CoV-2 infection. Symptoms include breathlessness, cough, chest tightness, palpitations, fatigue, myalgia, and difficulty concentrating. Estimates of 30% who contracted COVID-19 may experience Long COVID and 10% remain positive after 6 months post infection. Recent studies showed increased odds of Long COVID in RA though uncertainty remains on whether this was due to a direct response to infection or the natural RA symptom course. We set out to examine if characteristics and symptoms of those receiving Long COVID diagnosis appeared before COVID infection.
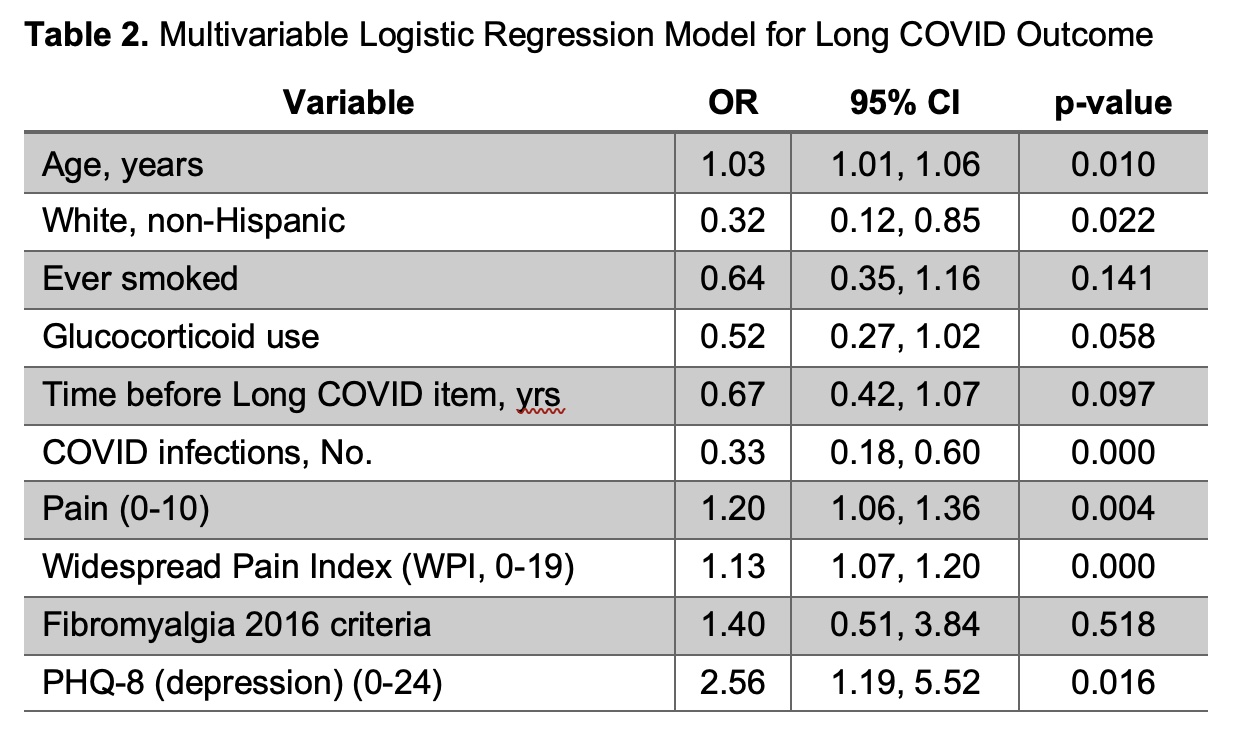
Methods: Data are from the FORWARD, The National Databank for Rheumatic Diseases, through comprehensive questionnaires collected from participants with physician-diagnosed RA and self-reported COVID infections at 6-month intervals through April 2023. Study inclusion required a response to the following Long COVID item: “Have you EVER been told by a healthcare provider that you have Long COVID?” first available July 2022. Baseline was defined as the survey closest to and before initial COVID infection or initial Long COVID if no prior COVID infection was reported. Respondents provided health information including socioeconomic status, treatments, symptoms, hospitalizations, and several PROs including HAQ, Fatigue, Pain, Sleep Problem, Health Satisfaction, PHQ-8 (depressive symptoms), GAD2 (anxiety symptoms), WPI, SSS, and fibromyalgia 2016 criteria. Descriptive analyses examined PROs at baseline according to future Long COVID status. A Lasso approach was used for variable selection in a multivariate logistic model with Long COVID as the outcome (presented using OR 95%CI).
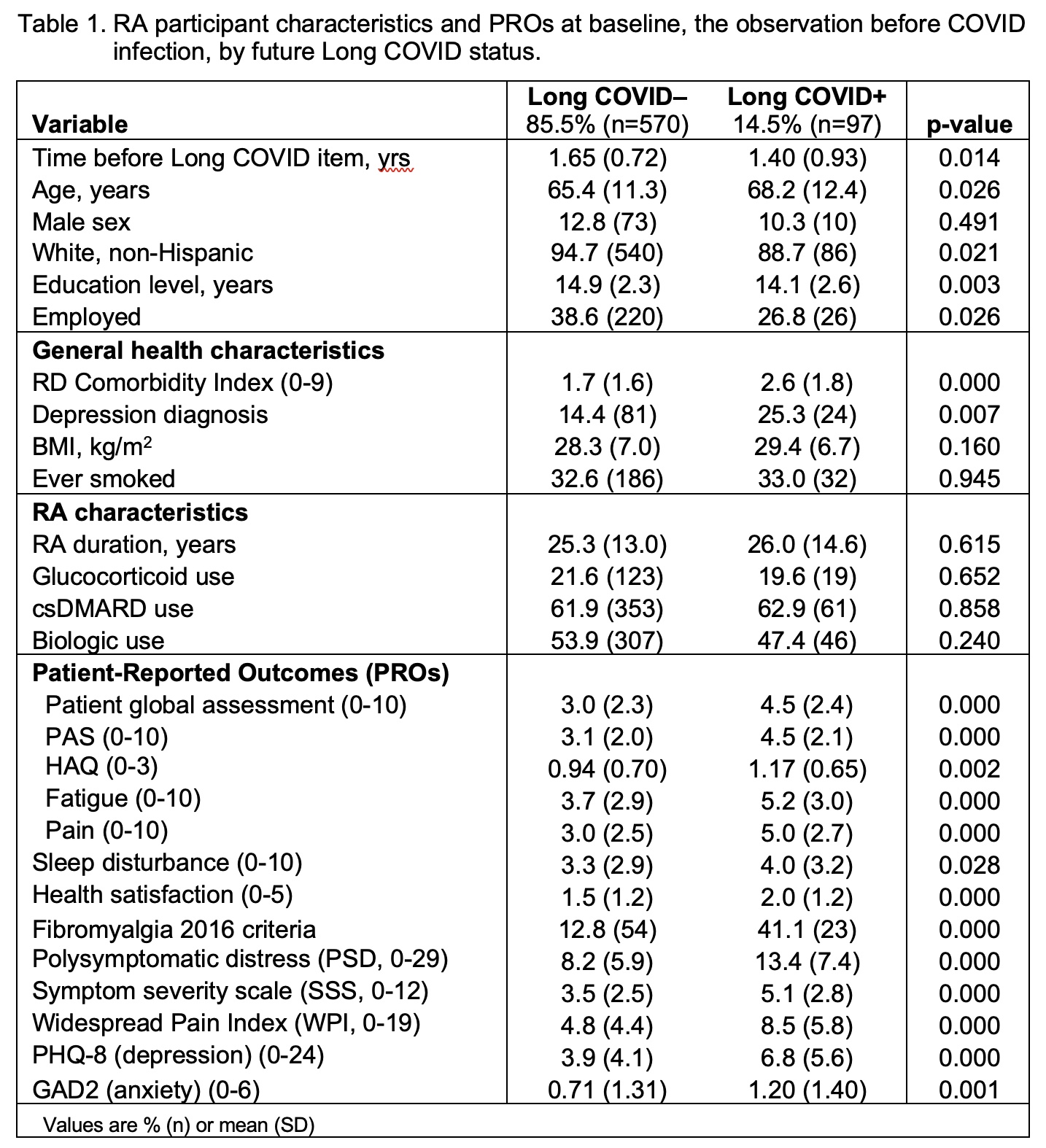
Results: There were 667 participants with RA, COVID infection, and who responded to the Long COVID item with 15% Long COVID positive. Those with Long COVID were older, less likely to be white, lower socioeconomic status, had more comorbidities, had worse RA PROs, more depression, more likely to meet fibromyalgia 2016 criteria, yet had no differences in DMARD use (Table 1). Fibromyalgia was ~3 times more common among those who would report Long COVID (13 vs 41%). Long COVID+ had more severe COVID infections with greater use of IV antibiotics (23% vs 9%) and hospitalizations for COVID (18 vs 5%). Multivariable logistic model had ten items after Lasso selection with several overlapping patient reported outcomes around pain and symptoms (Table 2).
Conclusion: Persons with RA who reported Long COVID in the past year had many symptoms of Long COVID prior to the development of a COVID infection. They had increases in many variables associated with RA severity and psychosocial distress. A Long COVID diagnosis may reflect preexisting illness, which may not be possible to separate. Our observations are limited by self-report and by not having official criteria for Long COVID diagnosis for healthcare providers. Future work will examine how well recent criteria identify Long COVID in our cohort, including those without COVID, and rates of Long COVID diagnosis termination.
To cite this abstract in AMA style:
Michaud K, Pedro S, Gandhi S, Wolfe F. Persons with Rheumatoid Arthritis and Long COVID Had Worse Pre-COVID RA Symptoms and Worse Non-RA Symptoms, as Well as Higher Rates of Fibromyalgia Compared with COVID Infected Long COVID Negative [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/persons-with-rheumatoid-arthritis-and-long-covid-had-worse-pre-covid-ra-symptoms-and-worse-non-ra-symptoms-as-well-as-higher-rates-of-fibromyalgia-compared-with-covid-infected-long-covid-negative/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/persons-with-rheumatoid-arthritis-and-long-covid-had-worse-pre-covid-ra-symptoms-and-worse-non-ra-symptoms-as-well-as-higher-rates-of-fibromyalgia-compared-with-covid-infected-long-covid-negative/