Session Information
Session Type: Abstract Session
Session Time: 3:00PM-4:30PM
Background/Purpose: Existing cardiovascular disease (CVD) risk calculators have inadequately estimated CVD risk in people with rheumatoid arthritis (RA). The American Heart Association (AHA) recently developed and validated the Predicting Risk of cardiovascular disease EVENTs (PREVENTTM) calculator, replacing the Pooled Cohort Equation (PCE) for estimation of CVD risk to inform primary prevention. Key updates include the removal of race, incorporation of renal function with recognition of the burden of cardiovascular-kidney-metabolic (CKM) syndrome, and estimation of heart failure (HF) risk in addition to atherosclerotic major adverse cardiovascular events (MACE). We evaluated the performance of PREVENTTM in RA vs. non-RA controls, and compared it to the PCE for predicting MACE in RA.
Methods: We identified US Veterans with RA (≥2 RA ICD-9/10 codes, rheumatologist diagnosis, and positive autoantibody or DMARD fill) between the ages of 30-79 years and matched them to up to 10 non-RA controls on age, sex, and VA enrollment year. Risk calculator components were derived from the VA Corporate Data Warehouse. Fatal and non-fatal MACE and HF events were identified using validated administrative algorithms in national VA, Medicare, and National Death Index data. Participants were excluded if they had pre-existing MACE or HF, missing risk calculator components, or risk factor values outside of validated ranges for the calculators. Estimated 10-year risk of MACE and HF was calculated according to published methods (Khan SS, et al. Circulation 2023; Yadlowsky S, et al. Ann Intern Med 2018), truncating follow-up at 10 years and adjusting risk proportionally for follow-up time < 10 years. Calibration (standardized incidence ratios [SIR; observed:expected events], calibration plots) and discrimination (Harrell’s C statistic) were assessed for each calculator. Performance of PREVENTTM in predicting overall CVD, MACE, and HF was compared in RA vs. non-RA controls. We subsequently compared performance of PREVENTTM vs. PCE for the prediction of MACE in RA.
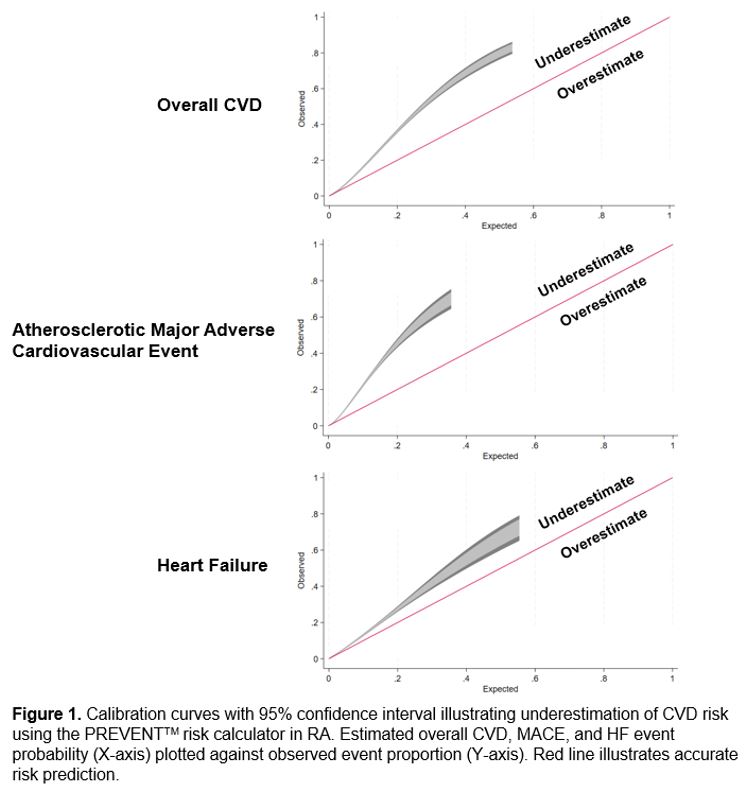
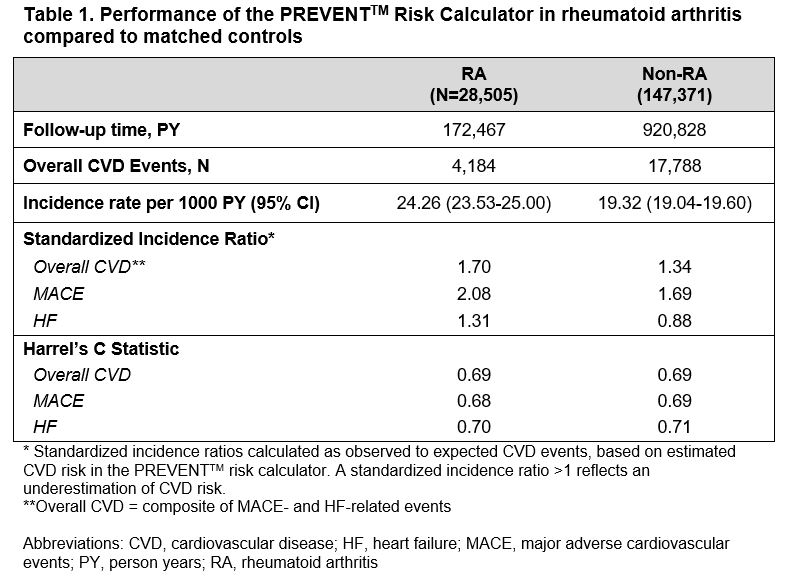
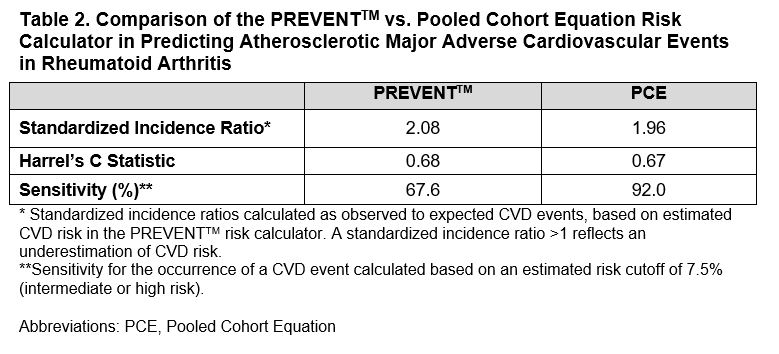
Results: We studied 28,505 patients with RA and 147,371 non-RA controls (mean age 62 years, 86% male). Over 1,093,295 person years of follow-up, CVD events occurred among 4,184 CVD RA (24.6 per 1000 PY) and 17,788 non-RA patients (19.3 per 1000 PY). The PREVENTTM calculator underestimated risk of all CVD outcomes in RA (Figure 1) and to a greater degree in RA compared to non-RA controls (Table 1; overall CVD: SIR 1.70 vs. 1.34; MACE: SIR 2.08 vs. 1.69; HF: 1.31 vs. 0.88). Discrimination was similar between RA and non-RA for all outcomes (Harrell’s C statistic range: 0.68-0.71). MACE prediction performance was similar in PREVENTTM compared to the PCE, with the exception of lower sensitivity among intermediate/high-risk individuals (risk >7.5%) in PREVENTTM (67.6% vs. 92.0%; Table 2).
Conclusion: In a large, national cohort of RA and matched non-RA patients, the novel AHA PREVENTTM risk calculator underestimated MACE and HF risk in RA. Building on suboptimal performance observed with prior CVD risk calculators in RA, these findings demonstrate the ongoing need to improve CVD risk prediction in RA.
To cite this abstract in AMA style:
Johnson T, Frideres H, Roul P, Yang Y, Baker J, brian S, Cannon g, Mikuls T, England B. Performance of a Novel Cardiovascular Risk Calculator in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/performance-of-a-novel-cardiovascular-risk-calculator-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/performance-of-a-novel-cardiovascular-risk-calculator-in-rheumatoid-arthritis/