Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The aim of this study was to utilize a machine learning (ML) approach to identify phenotypes of knee OA (KOA) based on demographic variables, symptoms, radiographs, and ultrasound (US) features.
Methods: We used data from participants enrolled in the population-based Johnston County Health Study (JoCoHS), who provided demographic and clinical information, symptomatic and functional assessments, and imaging (knee US and multiple joint radiographs). These data, minus the US results, were transformed, standardized, and combined into one set of measurements – the clinical data block. US images of each participant were obtained by a trained sonographer and scored independently by two expert readers, with any necessary adjudication by a third, independent reader. US features – including effusion/synovitis (0-3), medial and lateral osteophytes (0-3), meniscal extrusion (0-1), and articular cartilage damage (0-3) – made up the second block. The ML approach was based on the Angle-based Joint and Individual Variation Explained (AJIVE) algorithm, which aims to find shared (i.e., common to both data blocks) and individual (i.e., specific to each block) modes of variation. Here, we focused on shared structure to explore how US features and non-US clinical data vary together. We utilized loading plots to visualize the amount that each US and non-US variable contributed to a given mode of variation.
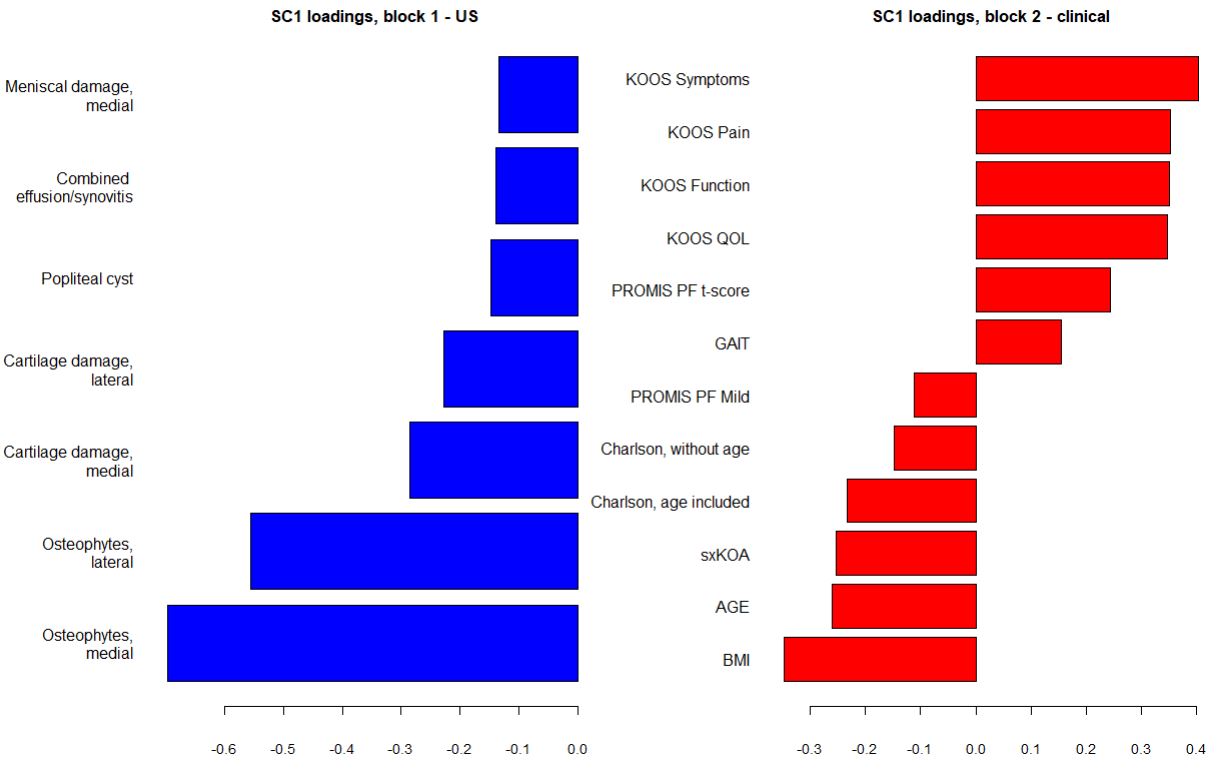
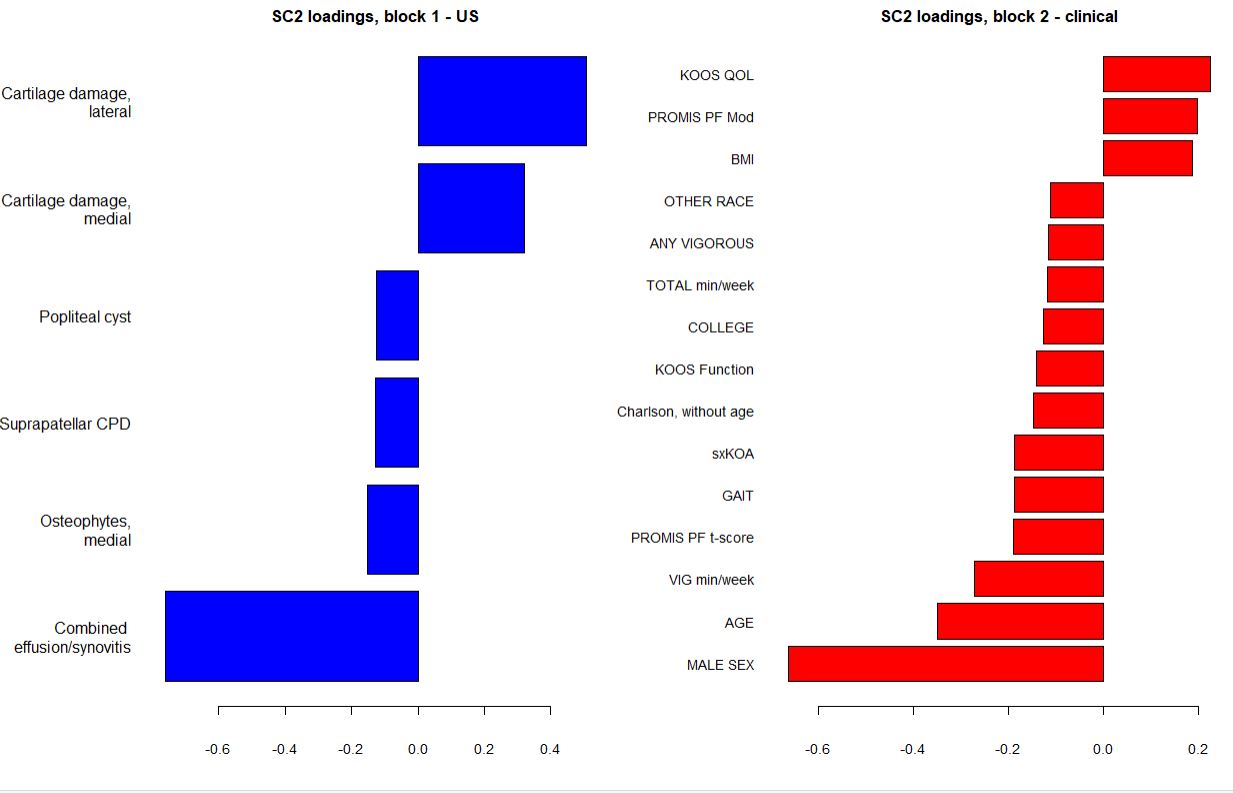
Results: This cross-sectional analysis included 500 JoCoHS participants (mean age 55 years, mean BMI 33 kg/m2, 65% women, 26% Black, 9% Hispanic), with (31%) and without (69%) KOA (defined as a Kellgren-Lawrence grade of 2 or more). We found two components of shared variation (Shared Components SC1 and SC2). The figures show the results as loadings onto the shared direction for each feature in two blocks, sorted by descending values.
SC1 demonstrated that the presence of osteophytes and cartilage damage on US (Figure 1A) was associated with higher BMI, older age, more symptomatic KOA, higher Charlson Comorbidity Index, and worse Knee Injury and Osteoarthritis Outcome (KOOS) scores (Figure 1B).
SC2 was characterized by presence of effusion and synovitis and less cartilage damage (Figure 2A). Clinical features associated with variation in this direction included more exercise per week, better physical function, lower BMI, male sex, and older age. (Figure 2B).
Conclusion: We identified two directions of shared of variation that represent two patterns or potentially different phenotypes of KOA. The first shared direction is consistent with prior studies which have linked presence of osteophytes and cartilage damage to worse symptoms and function in knee OA. Interestingly, the second shared direction appears to represent a more inflammatory type of KOA, with presence of effusion and synovitis but with less cartilage damage. This phenotype suggests earlier and less severe stages of OA. These different, clinically feasible phenotypes of knee OA should be confirmed in future studies.
BMI: Body Mass Index; sxKOA: symptomatic knee OA at the person level, at least one knee has both 1) any pain, aching, or stiffness on most days of any one month in past 12 months and 2) KLG of 2 or more; PF: Physical Function; PROMIS PF Mid: PROMIS-PF t score that is mild or worse (45 or less) from Health Measures reference; GAIT: gait in meter/second from the 8 foot walk, average of 2 trials used; PROMIS PF t-score: version 10a, lower is worse, t-score is standardized score where with mean=50 and SD=10; KOOS: The Knee Injury and Osteoarthritis Outcome Score; QOL: Quality Of Life.
VIG min/week: from the BRFSS, total minutes of vigorous (causing large increases in breathing or heart rate) activity per week for at least 10 minutes; PROMIS PF t-score: version 10a, lower is worse, t-score is standardized score where with mean=50 and SD=10; GAIT: gait in meter/second from the 8 foot walk, average of 2 trials used; sxKOA: symptomatic knee OA at the person level, at least one knee has both 1) any pain, aching, or stiffness on most days of any one month in past 12 months and 2) KLG of 2 or more; KOOS: The Knee Injury and Osteoarthritis Outcome Score; COLLEGE: college degree or higher; TOTAL min/week: from the BRFSS, total MVPA min/week defined as moderate min + 2(vigorous minutes); ANY VIGOROUS: On both BRFSS and IPAQ, at least 1 day/week of vigorous activity for at least 10 minutes.
To cite this abstract in AMA style:
Sawani S, Arbeeva L, Yates K, Alvarez C, Schwartz T, Savage-Guin S, Renner J, Bakewell C, Kohler M, Lin J, Samuels J, Nelson A. Patterns of Shared Variation in Knee Ultrasound for Osteoarthritis: A Machine Learning Approach [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/patterns-of-shared-variation-in-knee-ultrasound-for-osteoarthritis-a-machine-learning-approach/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patterns-of-shared-variation-in-knee-ultrasound-for-osteoarthritis-a-machine-learning-approach/