Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Although the increasing availability of biologic disease-modifying antirheumatic drugs (bDMARDs) and targeted synthetic DMARDs (tsDMARDs) has significantly improved outcomes for patients with Juvenile Idiopathic Arthritis (JIA), a substantial proportion of patients do not respond to an initial therapy, requiring switching to a second bDMARD/tsDMARD. Subsequent treatment decisions for children with continuing disease activity are haphazard, following a “trial and error approach”. The objective of this study is to characterize patterns of bDMARD/tsDMARDswitching among patients with JIA in real-world clinical settings following the initial bDMARD/tsDMARD therapy.
Methods: We conducted a retrospective study of a national administrative claims database in the US (January 2008 to March 2020). Study subjects included children (age < 19 years) who initiated a new bDMARD/tsDMARD therapy, had a medical claim associated with JIA diagnosis, and had been enrolled in the health plans for at least 6 months prior to starting initial bDMARD/tsDMARD therapy. Medications of interest comprised tumor necrosis factor inhibitors (TNFis), abatacept, tocilizumab, anakinra, canakinumab, tofacitinib, ustekinumab, rituximab, and secukinumab.
Results: 2,076 eligible children with JIA were prescribed bDMARD/tsDMARD therapy, most of whom started with TNFis (91%) (Table 1). Median follow-up was 699 days following first reported bDMARD/tsDMARD prescription (IQR 289-1503). During follow-up, 644 (31%) switched to a second bDMARD/tsDMARD, most commonly to a second TNFi (76%). A further 203 (9.8%) switched to a third bDMARD/tsDMARD and 30 (1.4%) patients received 4 or more bDMARD/tsDMARD therapies. The median time to initiating a second and third bDMARD/tsDMARD were 345 days (IQR 160-835) and 770 days (IQR 395-1435), respectively.
1,745 patients were followed-up for at least 180 days following start of the initial bDMARD/tsDMARD therapy, or switched to a second bDMARD/tsDMARD within 180 days. Among these patients, 193 (11%) started a second bDMARD/tsDMARD within 180 days of the initial therapy (i.e. early switchers). 88% of these patients received TNFi as the initial therapy and 76% switched to another TNFi. Children older than 12 years were more likely to be early switchers, compared with younger children (OR 1.05; 95% CI 1.02-1.08; p< 0.001).
The proportion of early switchers did not vary significantly over the study period. However, changes in the types of bDMARD/tsDMARD used were observed. Notably, there was a significant reduction in the use of TNFi as initial (from 95% in 2008-2010 to 86% in 2017-2020; p< 0.001), second (from 83% in 2008-2010 to 66% in 2017-2020; p< 0.001), and third therapy (from 56% in 2008-2010 to 29% in 2017-2020; p=0.010). There was also a significant trend towards increased use of tocilizumab and other bDMARD/tsDMARD as initial and subsequent therapies (Fig 1).
Conclusion: For many children with JIA, sequential use of bDMARD/tsDMARD is common. One-third of patients in our cohort received a second therapy and one in ten patients switched within 6 months of the initial therapy. More research is needed to evaluate the outcomes and optimal sequence of therapies in this population.
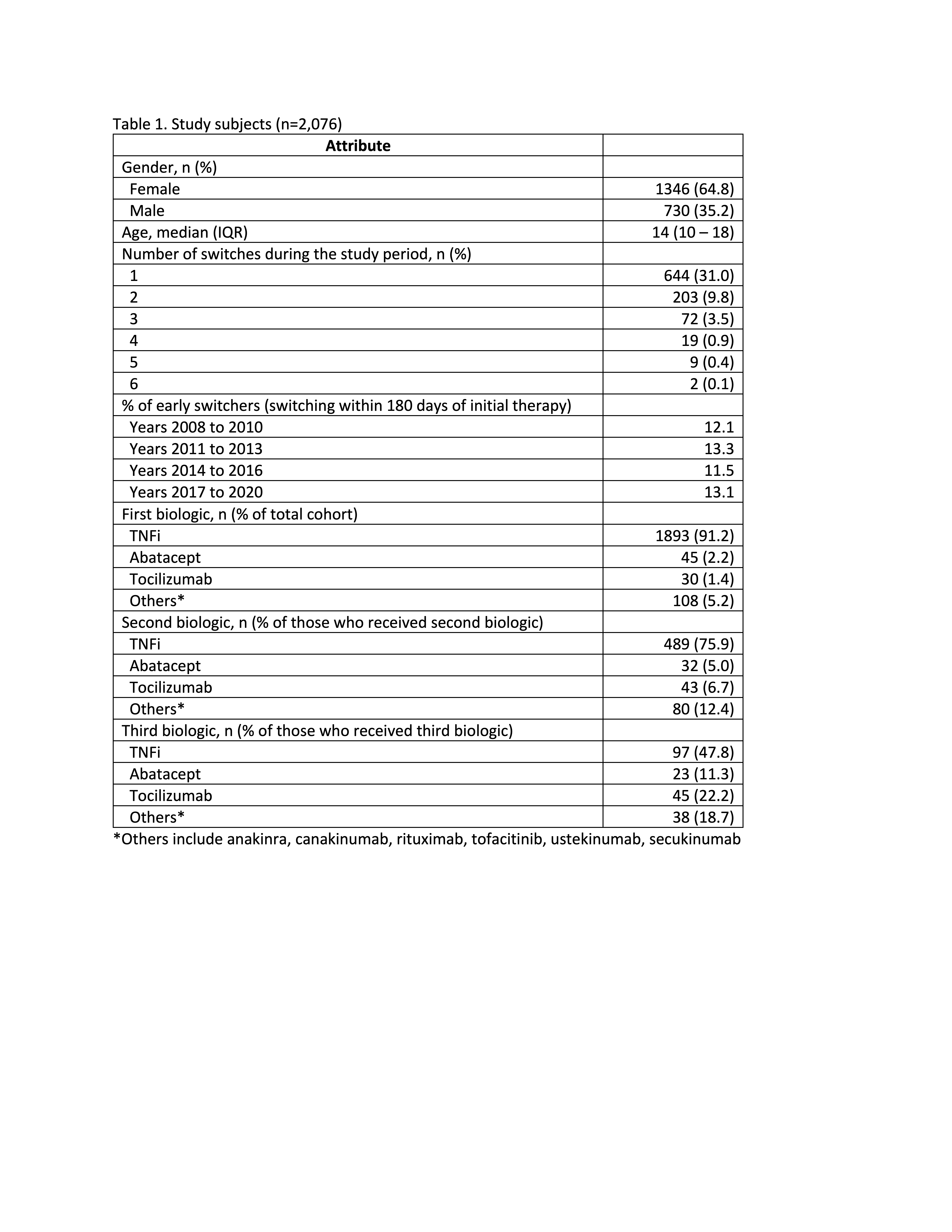 table1.jpeg”
table1.jpeg”
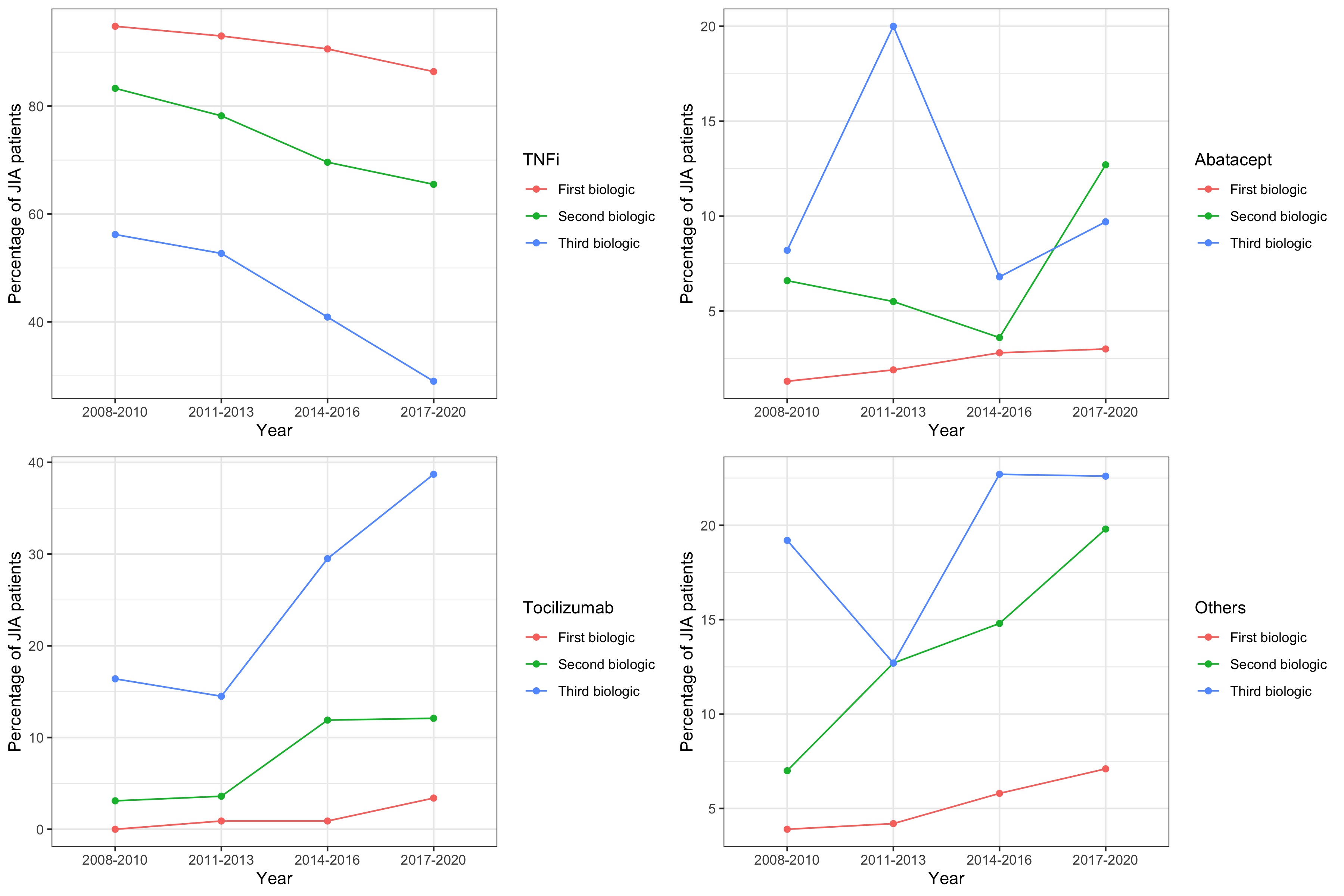 fig1.jpeg”
fig1.jpeg”
To cite this abstract in AMA style:
Ong M, Ringold S, Mannion M, Natter M, Schanberg L, Kimura Y. Patterns of Medication Switching in Juvenile Idiopathic Arthritis: A Retrospective Analysis of a National Administrative Claims Database [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/patterns-of-medication-switching-in-juvenile-idiopathic-arthritis-a-retrospective-analysis-of-a-national-administrative-claims-database/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patterns-of-medication-switching-in-juvenile-idiopathic-arthritis-a-retrospective-analysis-of-a-national-administrative-claims-database/