Session Information
Date: Monday, November 9, 2020
Title: RA – Diagnosis, Manifestations, & Outcomes Poster IV: Lifespan of a Disease
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with rheumatoid arthritis (RA) have higher comorbid depression and/or fibromyalgia (FM) than the general population. A multidimensional health-assessment questionnaire (MDHAQ) includes two queries concerning depression that provide a depression index (MDHAQ-DEP) which gives similar results to 2 widely used depression scales, Patient Health Questionnaire-9 (PHQ-9) and Hospital Anxiety and Depression Scale (HADS-D)1. The MDHAQ also provides 2 other indices: 1. RAPID3 (routine assessment of patient index data) to assess clinical status with similar results to DAS28 and CDAI, 2. FAST3 (fibromyalgia assessment screening tool), with similar results to formal FM criteria. We analyzed routine care RA patients for scores for RAPID3, FAST3, MDHAQ-DEP and 2 depression scales, PHQ-9 and HADS-D.
Methods: RA patients in routine care in Barcelona, Spain completed an MDHAQ, which includes 0-10 scores for physical function (FN), pain (PN), patient global assessment (PATGL), fatigue (FT), 0-48 -report RA disease activity index (RADAI) painful joint count, 0-60 symptom checklist (SX), one of which is depression, and a query concerning depression in the patient friendly HAQ format, scored 0–3.3 to give a 0–9.9 psychological MDHAQ index. MDHAQ indices include 0–30 RAPID3=FN+PN+PATGL, 3 cumulative indices to screen for FM: 0-3 FAST3-P – 1 each for PN ≥6, RADAI≥16, and SX≥16 (2/3=FM), 0-3 FAST3-F – 1 each for FT≥6, RADAI≥16, and SX≥16 (2/3=FM), and 0-4 FAST4 – 1 each for PN≥6, FT≥6, RADAI≥16, and SX≥16 (3/4=FM) and MDHAQ-DEP, based on a positive response on the depression SX query (Yes/No) or a score of ≥2.2 on the HAQ-like depression scale. Patients also completed the 0-27 PHQ-9 (≥10=depression), and 0-21 HADS-D (≥8=depression) scales. We compared RA patients who were MDHAQ-DEP positive and negative according to demographic data, scores for MDHAQ measures, RAPID3 and FAST3 indices, and PHQ-9 and HADS-D depression scales, using Student t tests, Wilcoxon rank-sum tests, chi-square tests or Fisher’s exact tests as appropriate.
Results: Among 102 patients, mean age was 58.8 years, mean education level 11.8 years, and 82% were female (Table). Mean RAPID3 was 11.6 (moderate severity), including 8.9 in 68 DEP-negative versus 17.2 in 33 DEP-positive patients (p< 0.0001), with similar patterns for all component scores (Table). High or moderate severity was seen in 97% of DEP-positive versus 63% of DEP-negative patients. FM FAST3-P, FAST3-F, and FAST4 screening were positive in 52-64% of DEP-positive vs 15-19% of DEP-negative patients. Scores on PHQ-9 and HADS-D also differed significantly in the 2 groups (Table, p< 0.0001).
Conclusion: RA patients positive for depression showed higher mean RAPID3 and FAST indices for FM. These associations must be considered in interpreting RAPID3 scores in clinical care in relation to treat-to-target recommendations.
Reference: 1. Morlà R et al. Arthritis Rheumatol. 2019; 71 (suppl 10).
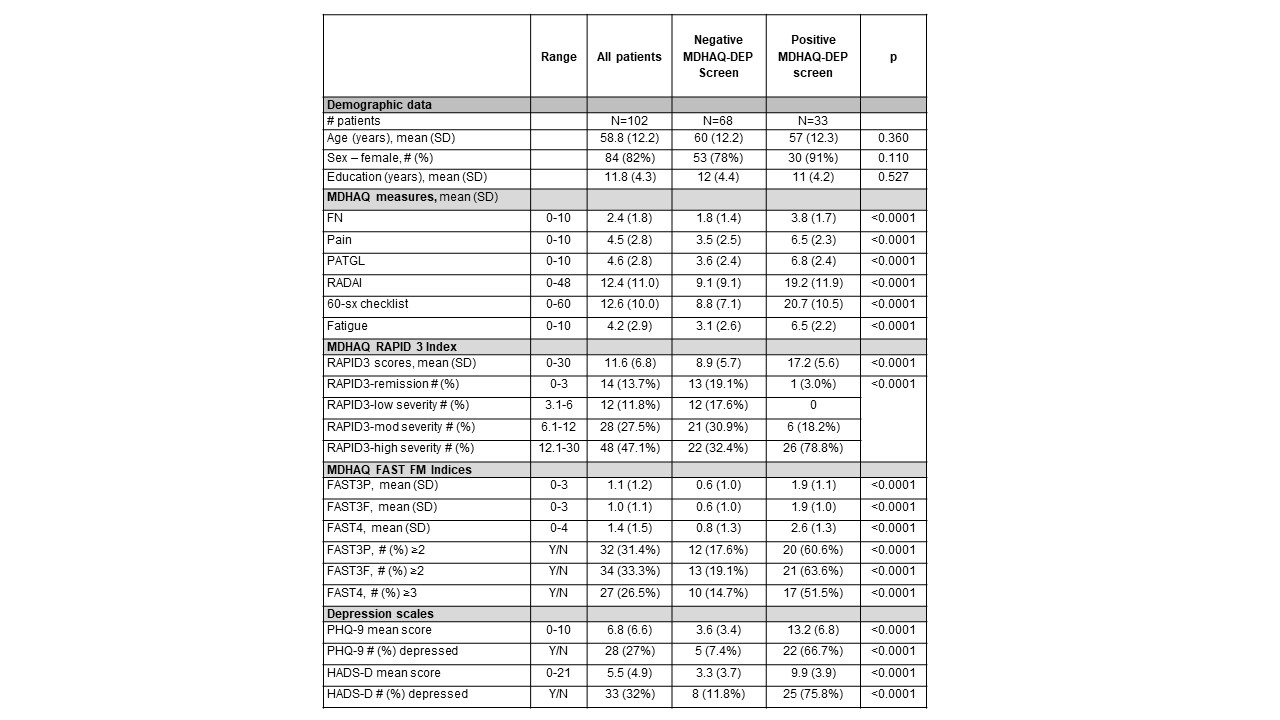 Table. Mean scores and # of RA patients according to MDHAQ depression (MDHAQ-DEP) negative or positive status
Table. Mean scores and # of RA patients according to MDHAQ depression (MDHAQ-DEP) negative or positive status
To cite this abstract in AMA style:
Morlà R, Li T, Inciarte-Mundo J, Castrejon Fernandez I, Gómez-Puerta J, Sanmartí R, Pincus T. Patients with Rheumatoid Arthritis and Comorbid Depression Have High Levels of RAPID3 (Routine Assessment of Patient Index Data) and FAST3 (Fibromyalgia Assessment Screening Index) on a Multidimensional Health Assessment Questionnaire (MDHAQ) [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/patients-with-rheumatoid-arthritis-and-comorbid-depression-have-high-levels-of-rapid3-routine-assessment-of-patient-index-data-and-fast3-fibromyalgia-assessment-screening-index-on-a-multidimension/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patients-with-rheumatoid-arthritis-and-comorbid-depression-have-high-levels-of-rapid3-routine-assessment-of-patient-index-data-and-fast3-fibromyalgia-assessment-screening-index-on-a-multidimension/