Session Information
Date: Saturday, November 12, 2022
Title: SLE – Diagnosis, Manifestations, and Outcomes Poster I: Diagnosis
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Cardiac magnetic resonance imaging (cMRI) is the gold standard modality for evaluation of cardiac anatomy, function, and characterization of myocardial tissues. cMRI has been proposed to be helpful in SLE patients to distinguish between myocardial inflammation, suspected infiltration, perfusion abnormalities, and fibrosis. No practice guidelines currently exist to provide specific recommendations for cMRI in SLE patients. Using a large, de-identified electronic health record (EHR), we examined ordering practices of cMRI in SLE patients and its impact on clinical care.
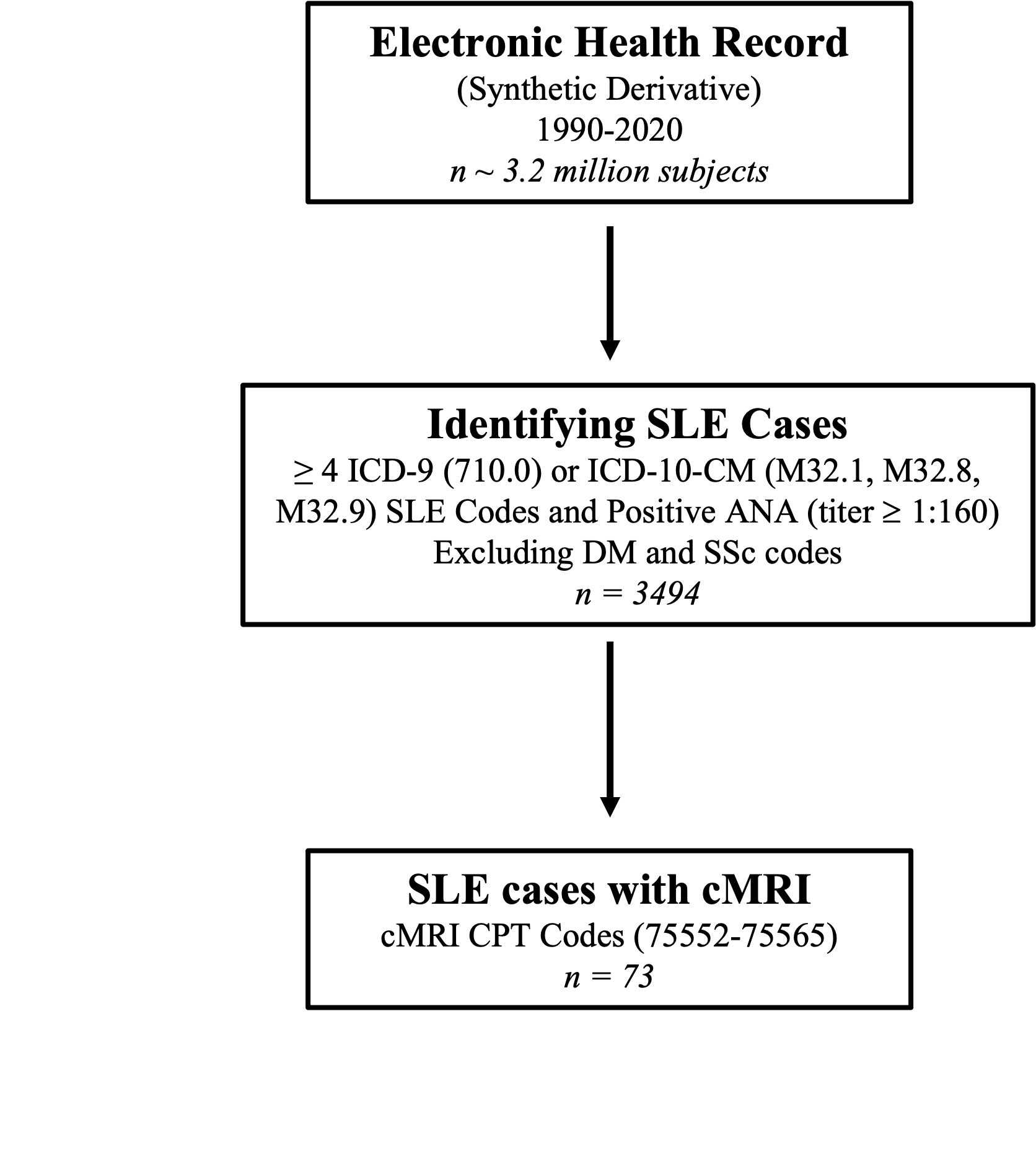
Methods: SLE patients were identified from a de-identified EHR with over 3.4 million subjects with over 30 years of follow-up using a previously validated algorithm. Within this SLE cohort (n = 3494), we used CPT codes 75552-75565 to identify SLE patients with cMRIs (Figure 1). Demographic and clinical information were obtained from chart review.
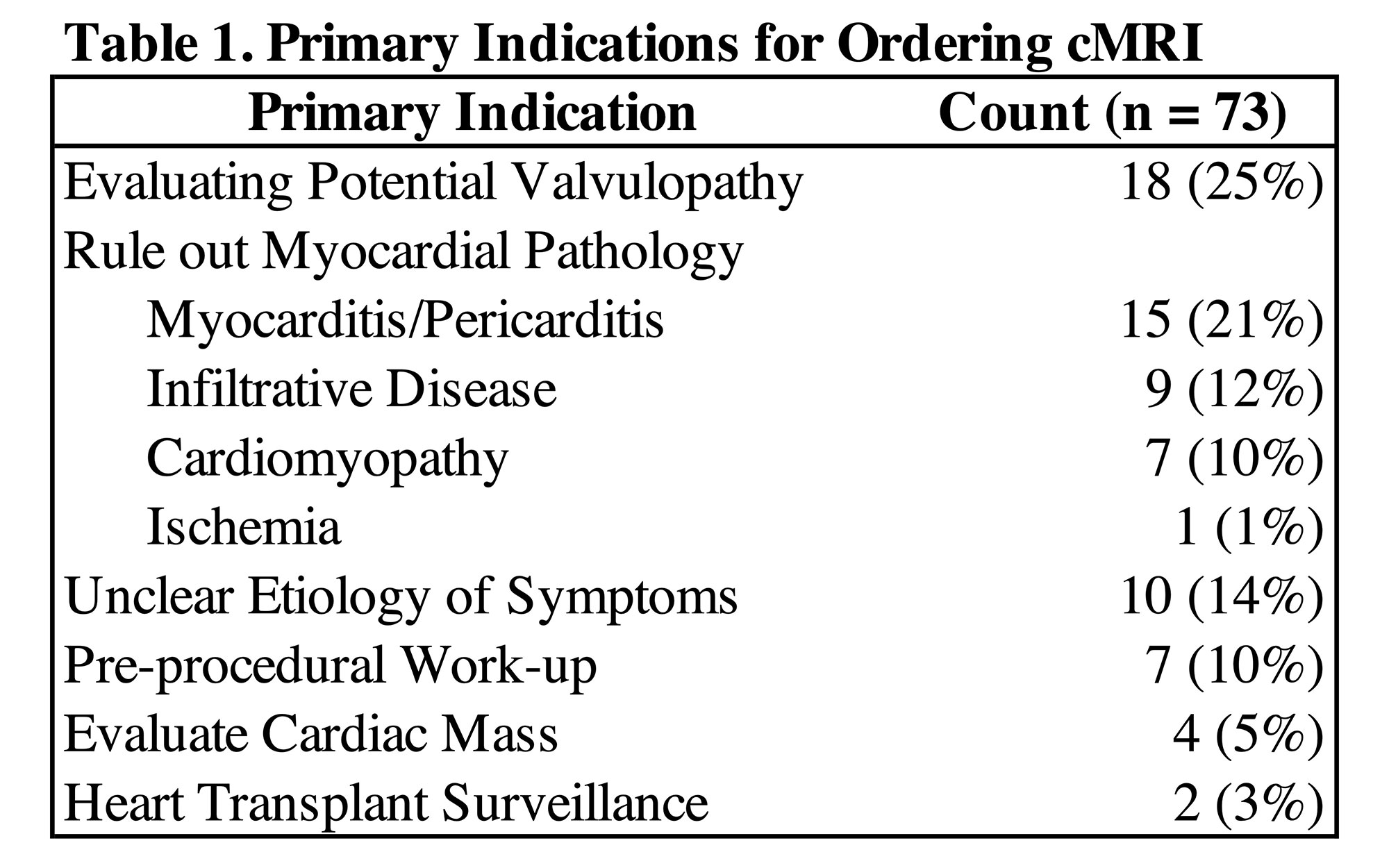
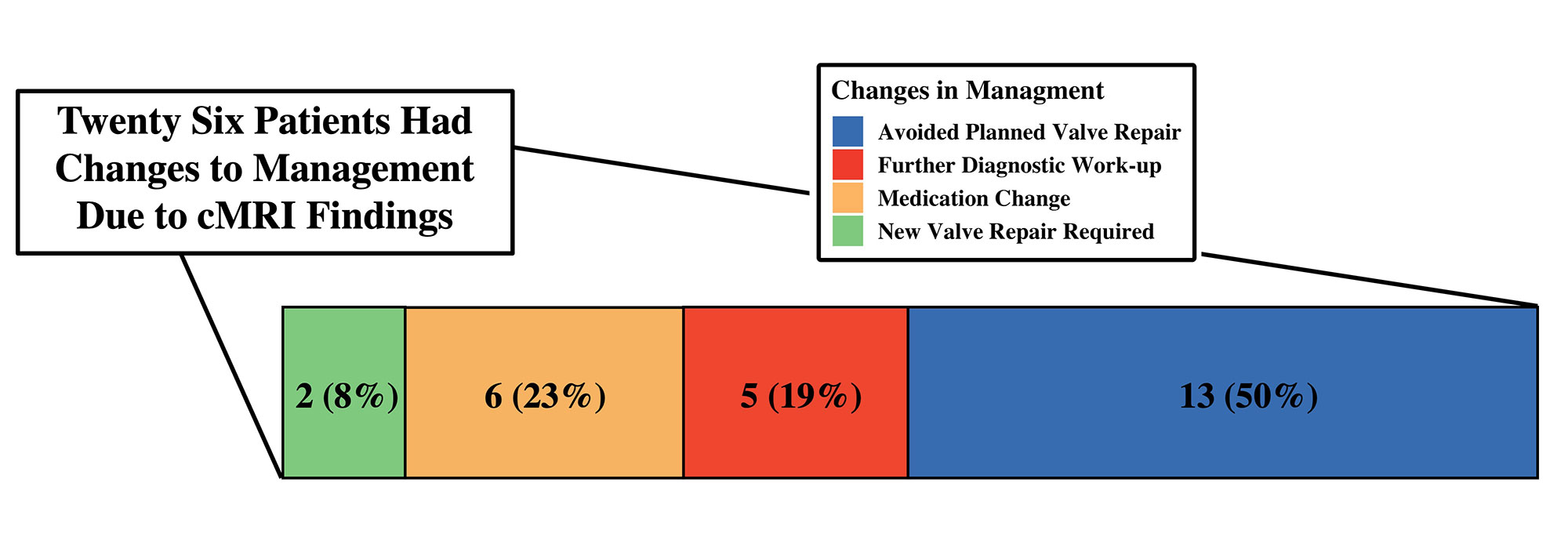
Results: There were 73 SLE patients (90% female, 53% white) who underwent cMRI between 2005 and 2020. Of the cohort, 67 (92%) had cardiopulmonary symptoms while 6 (8%) patients were asymptomatic. Of the patients with symptoms, all had prior electrocardiograms and 82% had transthoracic echocardiogram (TTE), 12% stress test, 16% left heart catherization, and 11% right heart catherization prior to a cMRI. Indications for ordering cMRI are displayed in Table 1. Of the 42 cMRIs ordered to evaluate myocardial pathology or unclear cardiopulmonary symptoms, 31 (74%) were ordered to follow up on pathology seen on TTE and 11 (26%) to evaluate for pathology not seen on TTE. There were 12 cMRIs that raised concern for a pathologic process not previously considered, of which 3 led to biopsies and final diagnosis of either amyloid or myocarditis. Of 18 patients who underwent cMRI to evaluate severity of valvular pathology, 13 (72%) avoided a planned valve repair. Of the 73 total cMRI ordered, 26 (35%) led to management changes including 2 patients requiring valve repair, 6 patients requiring medication changes, 5 patients requiring further diagnostic work up, 13 patients avoiding planned valve repair (Figure 2). Only 15% of cMRIs were performed with the newer quantitative parametric mapping techniques.
Conclusion: In the majority of SLE patients, cMRIs were ordered to distinguish between myocarditis/pericarditis, infiltrative disease, cardiomyopathy, and ischemia as the underlying cause for cardiopulmonary symptoms. Although cMRIs are not commonly ordered in this patient population, the results of cMRIs changed management in a significant number of SLE patients. cMRIs were ordered to assess the degree of valvular pathology and were particularly helpful for avoiding surgical valve intervention. Advances in cMRI technology have increased diagnostic utility with future studies needed to determine its role in guiding immunosuppressive therapies for myocardial pathology.
To cite this abstract in AMA style:
Chew E, Varghese B, Chew C, Frech T, Wells Q, Barnado A. Ordering Practices and Diagnostic Utility of Cardiac MRI in SLE Patients at a Single Academic Institution [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/ordering-practices-and-diagnostic-utility-of-cardiac-mri-in-sle-patients-at-a-single-academic-institution/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/ordering-practices-and-diagnostic-utility-of-cardiac-mri-in-sle-patients-at-a-single-academic-institution/