Session Information
Session Type: Abstract Session
Session Time: 1:00PM-2:30PM
Background/Purpose: Precision medicine has previously identified subgroups of clinical trial participants with knee osteoarthritis (kOA) that benefit more from a specific intervention than others. We used a precision medicine approach in the Weight-Loss and Exercise for Communities with Arthritis in North Carolina (WE-CAN) data set comparing a diet and exercise intervention to an attention control to determine the optimal treatment regimen targeting WOMAC pain score in specific participants with kOA and overweight/obesity.
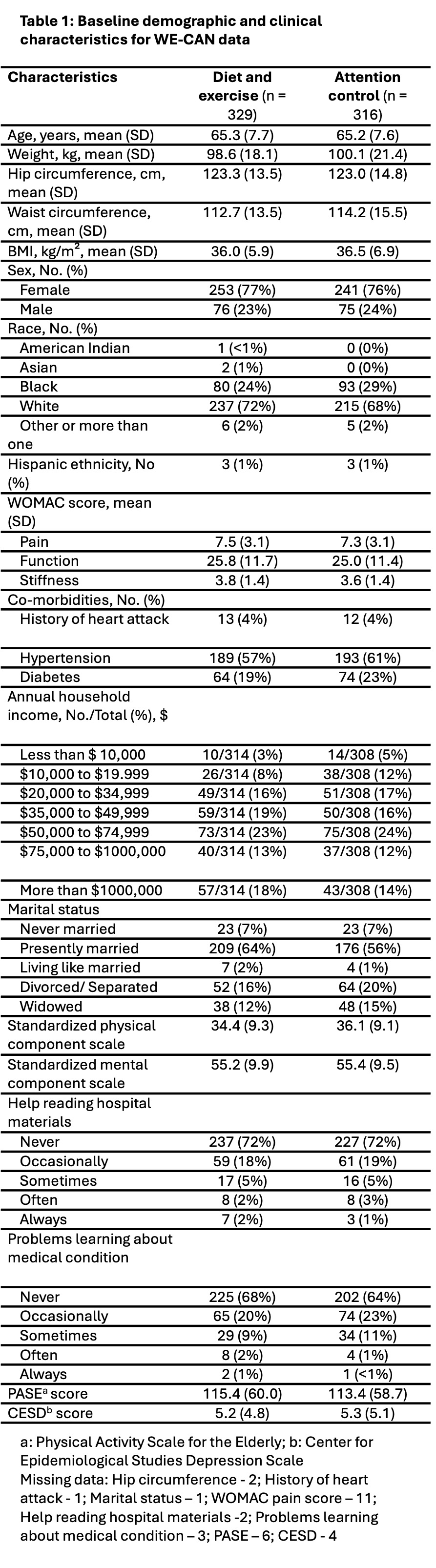
Methods: We used a subset of 645 out of 823 participants (i.e., those who were not missing outcome data) in the WE-CAN data set who were randomly assigned to either a diet and exercise intervention or an attention control (healthy lifestyle education group sessions) for 18 months (PMID 36511925). Based on clinical judgement and prior analyses of optimal kOA interventions, we selected baseline features, including demographics, physical features, WOMAC subscales, activity level, and comorbidities, which are included in Table 1. These were entered into 5 machine learning models and 2 fixed treatment models (zero-order models). Individualized treatment rules (ITRs) were estimated for change in WOMAC pain score at 18 months, and value functions were calculated for each ITR. A higher value function indicated a higher quality of the estimated ITR, signifying more benefit to future patients based on predicted WOMAC pain scores. Validation methods for this study included cross-validation and Jackknife Estimator.
Results: The average (standard deviation) age of participants was 65.3 (7.7) years, and the mean BMI was 36.3 (6.4) kg/m2 (Table 1). Most participants were women (76.6%), and most had co-morbidities, including obesity, hypertension, and arthritis in other joints. A smaller proportion had diabetes and/or cardiovascular disease. On a scale of 1-20, with larger numbers indicating more severe pain, the average baseline WOMAC pain score was 7.4.
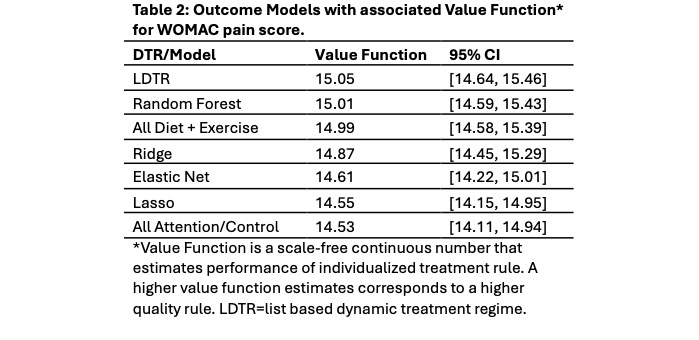
Value functions for each machine learning model regarding change in WOMAC pain scores are shown in Table 2. Placing all participants in the Diet and Exercise group (zero-order model) was among the highest value functions. We found no statistically significant subgroups that would benefit more from the alternative treatment (attention control).
Conclusion: In the WE-CAN study, precision medicine models found no significant improvement (i.e., small differences in value functions and overlapping confidence intervals) in pain scores over treating all participants with kOA with both diet and exercise. This supports the utility of the diet and exercise intervention in all patients with symptomatic kOA and overweight/obesity. Future work will evaluate additional features (depression and self-efficacy) and alternative outcomes, such as change in SF-36 physical component score, weight, WOMAC function/stiffness scores, compressive force, and plasma IL-6. The WE-CAN data set compared diet and exercise to an attention control group; therefore, the efficacy of precision models to predict response to alternative treatment options such as diet or exercise alone should continue to be researched in this and other studies.
To cite this abstract in AMA style:
Walton C, Hurley F, Arbeeva L, Messier S, Mihalko S, Katz J, Loeser R, Hunter D, Callahan L, Nelson A. Optimizing Knee Osteoarthritis Treatment with the Precision Medicine Approach in a Clinical Trial Dataset [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/optimizing-knee-osteoarthritis-treatment-with-the-precision-medicine-approach-in-a-clinical-trial-dataset/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/optimizing-knee-osteoarthritis-treatment-with-the-precision-medicine-approach-in-a-clinical-trial-dataset/