Session Information
Date: Sunday, November 12, 2023
Title: (0380–0422) RA – Diagnosis, Manifestations, and Outcomes Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Despite the diagnostic contribution of Anti-CCP3.1 (cyclic citrillunated peptide) antibody and RF (rheumatoid factor) as classified by the 2010 ACR/EULAR RA criteria, approximately one-third of patients with rheumatoid arthritis (RA) are considered “seronegative.” Novel markers, Anti-CarP Anti-Sa, and Anti-CEP1 were recently added in order to improve RA diagnosis and characterization. Citrullination and carbamylation are post-translational modifications, and autoantibodies against citrullinated and carbamylated proteins in RA patients may predict the development of RA and may be associated with more active disease and higher risk of developing joint erosions.
Methods: Serum from 28,575 patient samples was analyzed for RF (Roche Integra/COBAS), Anti-CCP3.1 (QUANTA Lite IgG/IgA), and/or enzyme immunosorbent assay (ELISA) lab-developed tests (LDT) for 14-3-3 eta, Anti-CarP, Anti-Sa, and/or Anti-CEP1 in three RA profiles: RheumAssure (RF, Anti-CCP3.1, 14-3-3 eta), RAdx6 (RF, Anti-CCP3.1, 14-3-3 eta, Anti-CarP, Anti-Sa, Anti-CEP1) and SeroNegRAdx4 (14-3-3 eta, Anti-CarP, Anti-Sa, Anti-CEP1).
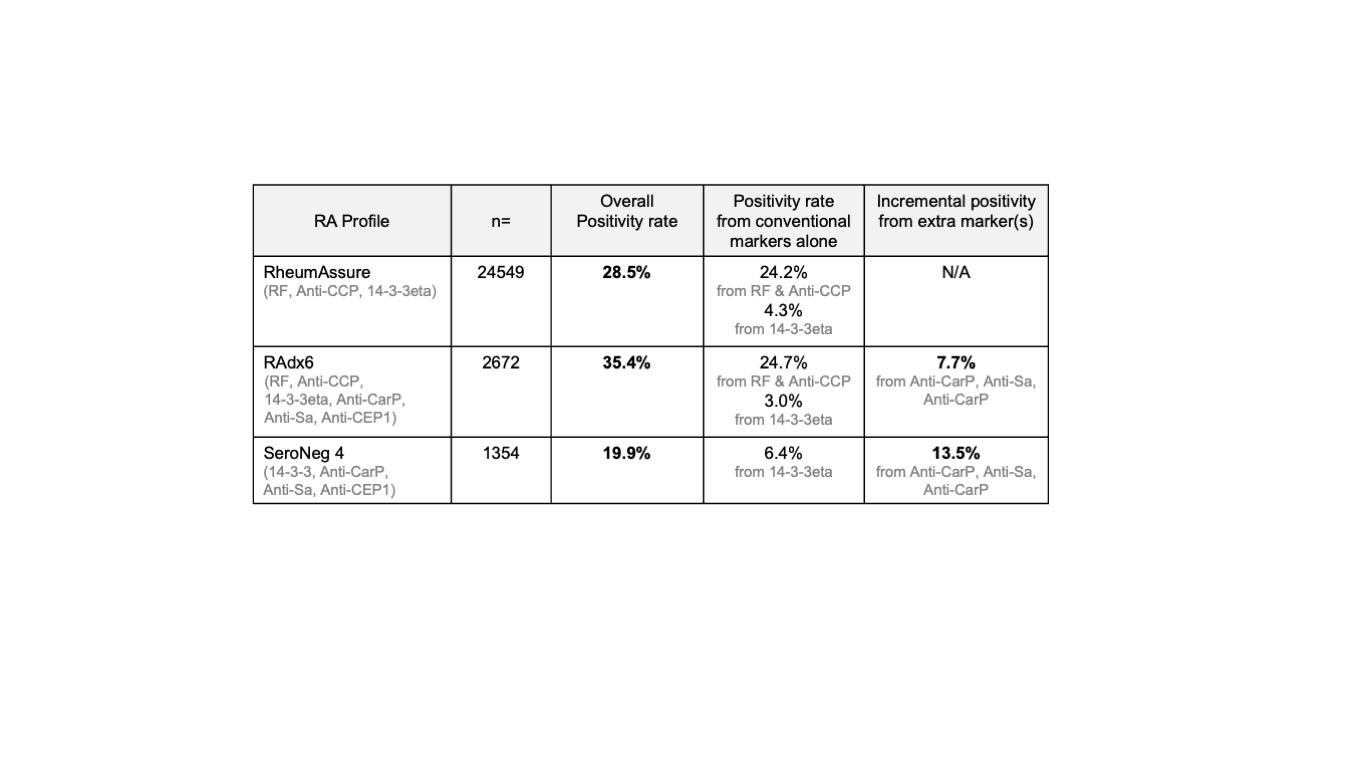
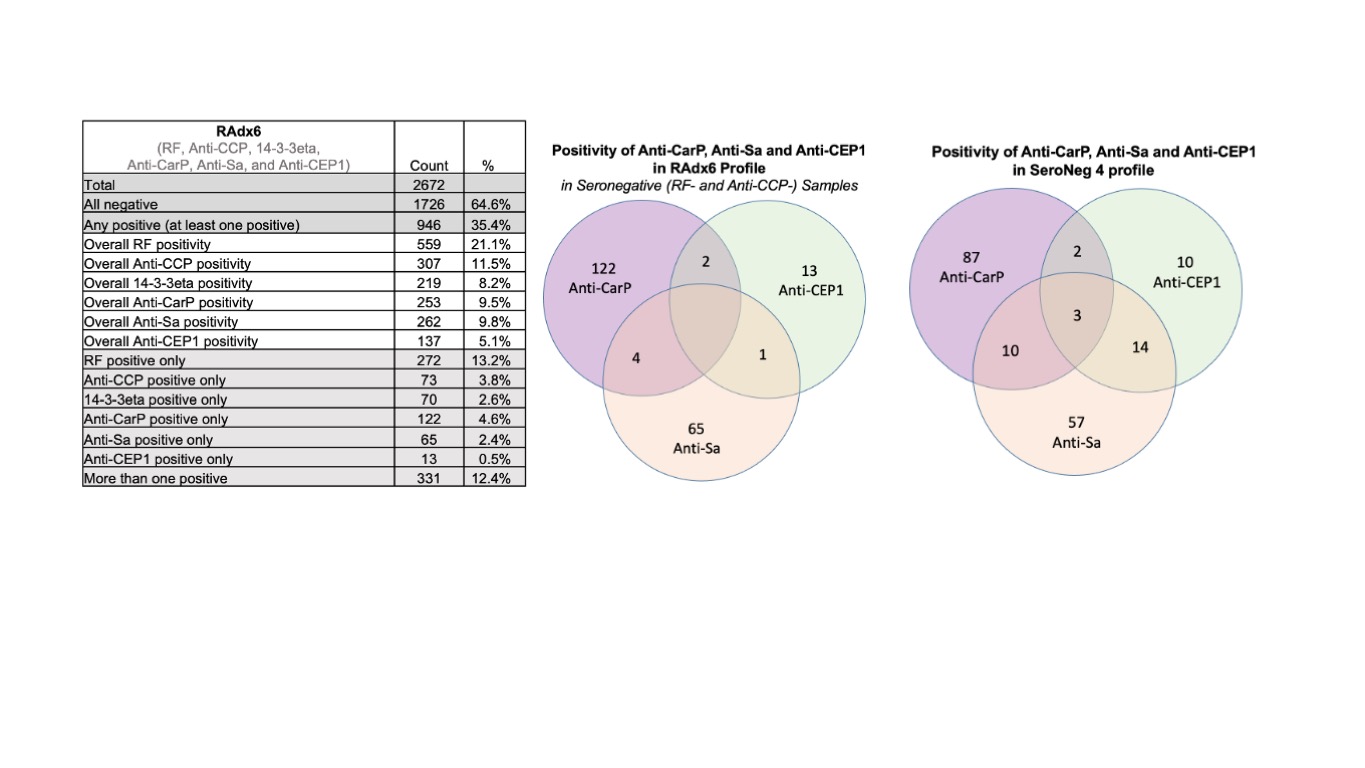
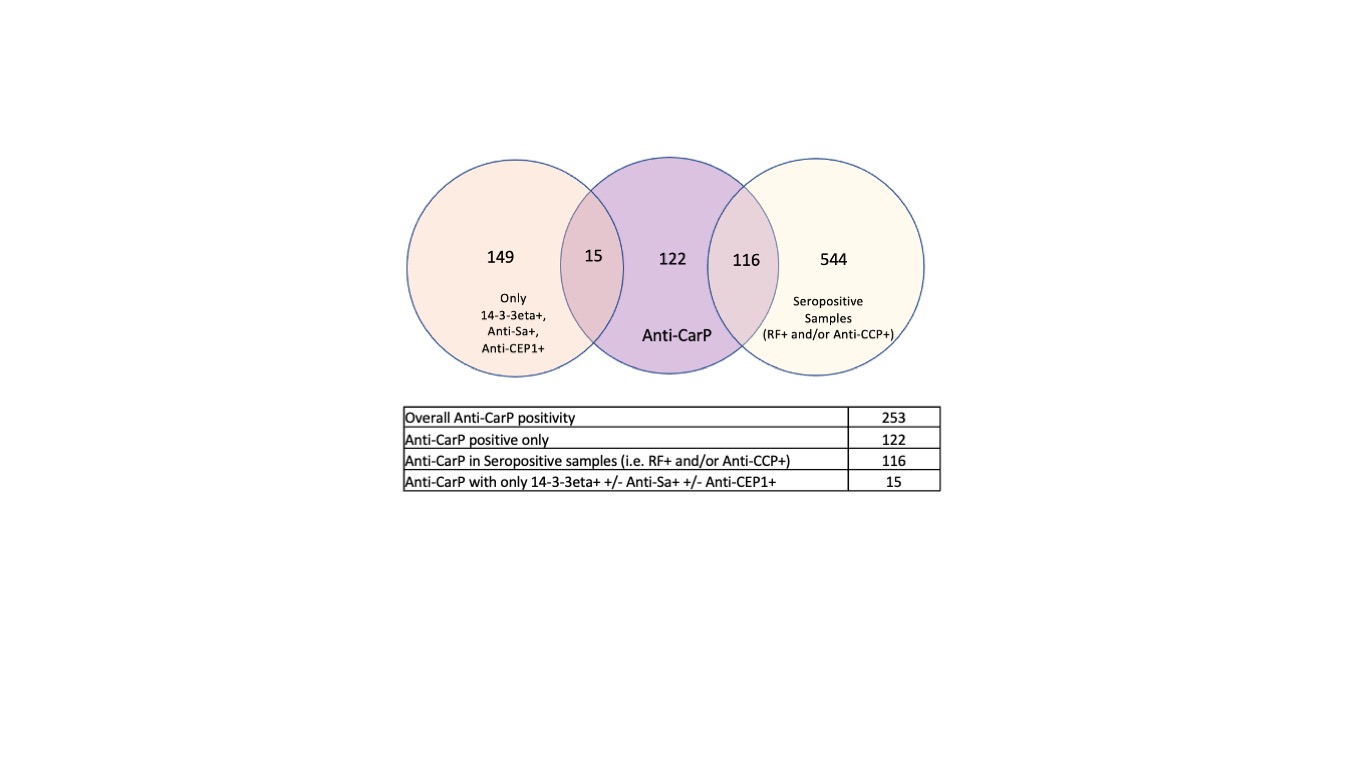
Results: Here, 24,549 RheumAssure, 2672 RAdx6 and 1354 SeroNegRAdx4 were performed and exhibited overall positivity of 28.5%, 35.4% and 19.9%, respectively as shown in Table 1. Novel markers, Anti-CarP, Anti-Sa and Anti-CEP1, added an incremental positivity of 7.7% and 13.5% in RAdx6 and SeroNegRAdx4, respectively. Of note, this additional 7.7% positivity was seen in 207 (of 2672 total) RAdx6 samples that tested negative for RF, Anti-CCP3.1 and 14-3-3 eta. SeroNegRAdx4 is designed to be useful in patients with high clinical suspicion for RA who have previously tested negative for RF and Anti-CCP. Though clinical histories are not known, almost twice as many, 13.5%, were positive for Anti-CarP and/or Anti-Sa and/or Anti-CEP1. In Table 2, positivity rates of individual markers in RAdx6 are shown where RF was the most frequently positive, followed by Anti-CCP3.1, Anti-Sa, Anti-CarP, 14-3-3 eta, and Anti-CEP1. Concomitant positivity of more than one marker was common, occurring in one third of all positives (331/946, 35.0%). Almost one-quarter (24.7%) of all RAdx6 samples were Seropositive (RF+ and/or Anti-CCP3.1+). In Seronegative samples, the positivity of Anti-CarP, Anti-Sa and Anti-CEP1 (Figures 1 and 2) may be helpful for diagnosis. Figure 3 shows that more than half the time, Anti-CarP is positive in the presence of another RA-specific marker (131/253, 51.8%).
Conclusion: Here, we show the overall positivity rates of three RA profiles. RAdx6 as the most comprehensive RA profile is positive more than one-third of the time. SeroNegRAdx4 offers a potential 20% incremental benefit in diagnosing RA. RF and Anti-CCP3.1 together can detect about a quarter of all positivity observed, but novel markers for RA, Anti-CarP, Anti-Sa and Anti-CEP1, provide additional positivity of 7.7% and 13.5% that may be beneficial in diagnosing early RA and RA in Seronegative patients. Anti-CarP was frequently positive with RF and/or Anti-CCP3.1 and as such, is a useful prognostic marker for erosive disease.
To cite this abstract in AMA style:
Yang J, Punzalan R, Andrew L, Nappi M, ricchiuti V, Zikry M, Chun K. Novel Diagnostic Markers for Rheumatoid Arthritis Including Anti-CarP (Carbamylated Protein), Anti-Sa (Citrullinated Vimentin) and Anti-CEP1 (Citrullinated Enolase Peptide1) Are Frequently Positive in Diagnostic Profiles [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/novel-diagnostic-markers-for-rheumatoid-arthritis-including-anti-carp-carbamylated-protein-anti-sa-citrullinated-vimentin-and-anti-cep1-citrullinated-enolase-peptide1-are-frequently-positive-in/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/novel-diagnostic-markers-for-rheumatoid-arthritis-including-anti-carp-carbamylated-protein-anti-sa-citrullinated-vimentin-and-anti-cep1-citrullinated-enolase-peptide1-are-frequently-positive-in/