Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Near infrared (NIR) imaging of indocyanine green (ICG) in rheumatoid arthritis (RA) models identified abnormal lymphatic vessel (LV) function, which can be quantified as ICG clearance from the injection site via longitudinal (days) NIR imaging. As the role of LV function in RA is unknown, we hypothesized that ICG clearance from hand web spaces and efferent LV contraction frequency of RA patients experiencing flare is significantly decreased compared to normal healthy volunteers. We also assessed the characteristics of filled LVs to examine if structural differences are present in RA lymphatics and healthy controls.
Methods: The web spaces of both hands of 12 healthy controls (CTL) and 7 subjects with RA flare (ACR 2010 RA criteria) were injected with 0.1ml of 100μM ICG on 2-4 separate occasions, and the hands underwent NIR imaging. To measure clearance of ICG from the web spaces, 7 CTL and 7 RA subjects were reimaged 7-9 or 13-15 days after the first injections, and the remaining NIR fluorescence was measured via region of interest (ROI) analysis (Paired t-test). Controlling for the number of days between subjects, the change in intensity between the initial and second visit was divided by the number of days between visits (t-test). Lymphatic contractions for LVs were determined from graphs of ROI intensity across time to calculate contractions per minute, and assessed via Wilcoxon Rank Test. To assess the branching structure of the vessels, manual segmentation of the lymphatic network and subsequent spatial mapping was performed (t-test). Then two independent graders quantified the total number of bifurcations of the LVs. Median values for each hand across all visits and graders were used to test for differences (Wilcoxon Rank-Sum Test).
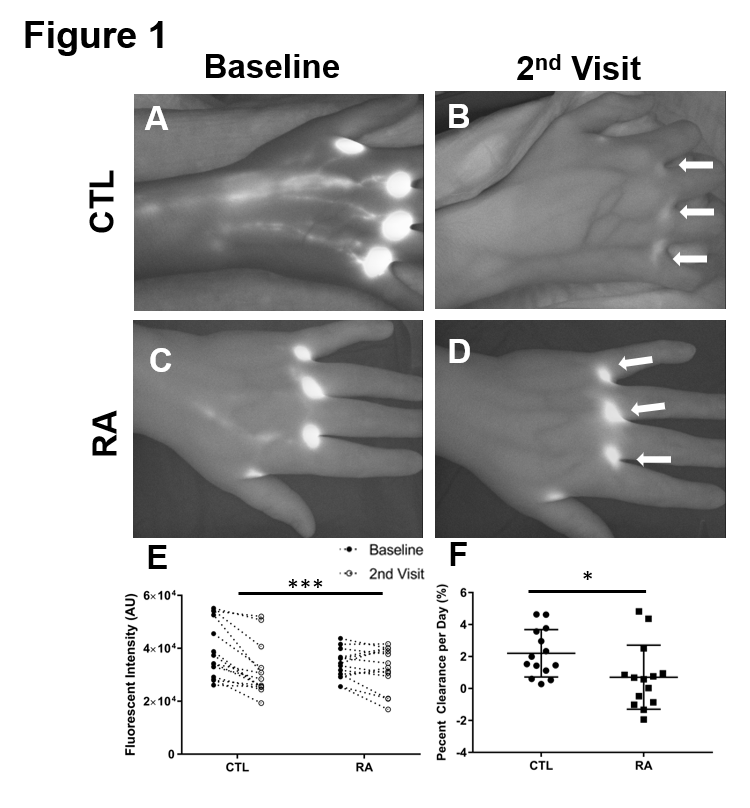
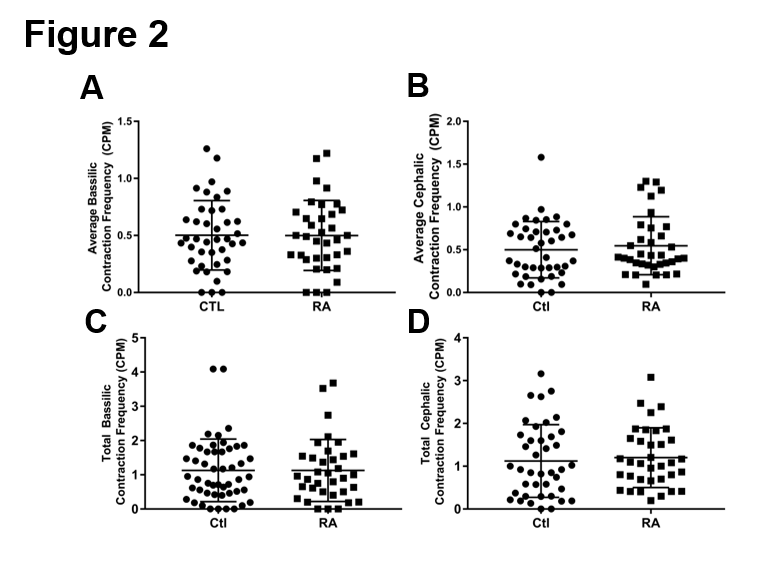
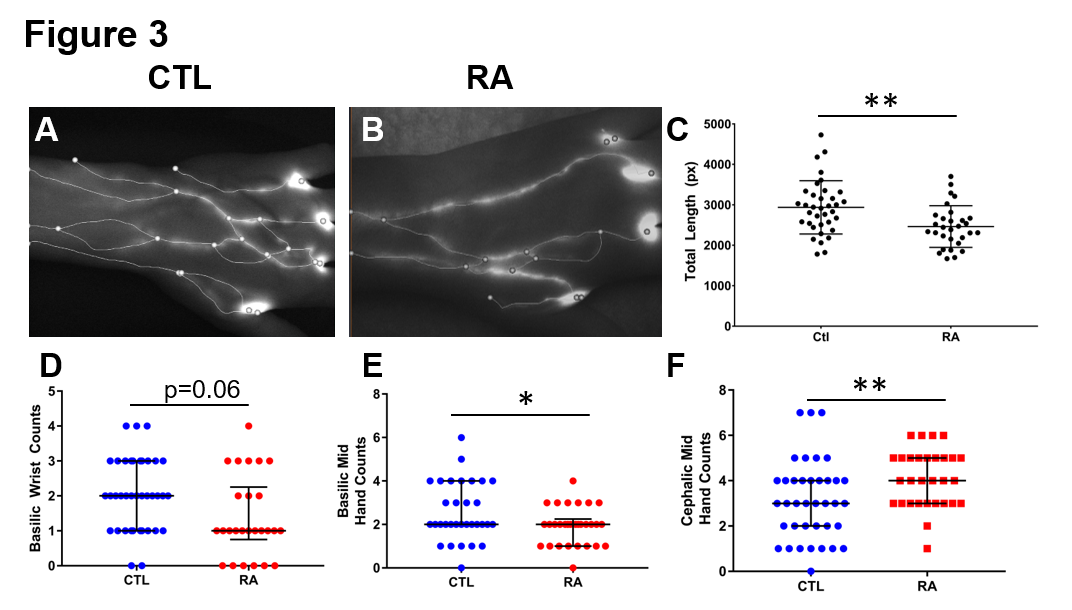
Results: Representative NIR images of CTL and RA hands at baseline, and at the second visit, demonstrate the dramatic retention of ICG at the injections sites (White Arrows) in RA subjects (Fig 1 A-D). Statistical analysis revealed a decrease in ICG clearance in the RA subjects vs. CTLs (Fig 1 E, ***p< 0.001). When controlling for days between the initial visit and second visit the relationship persisted (Fig 1F, *p< 0.05). Interestingly, no difference in contraction frequency was observed between CTLs and RA subjects (Fig 2A-D). However, there was significantly decreased total length in the spatial structure of the lymphatic network (Fig 3A-C, *p< 0.05). This decreased length was primarily attributed to a lack of basilic associated ICG filled vessels in RA subjects (Fig 3D-F, *p< 0.05).
Conclusion: Imaging outcomes of LV function in mice have demonstrated diminished clearance of lymph from inflamed joints during arthritic progression. Herein, we show a significant reduction in ICG clearance and altered anatomic structure in RA subjects’ hands during flare. The accumulation and retention of inflammatory cells and molecules in RA joints as a result of diminished lymphatic clearance may be a critical factor in the initiation and persistence of synovitis. This clinical pilot demonstrates the feasibility of quantifying LV function, and warrants formal investigation in clinical trials.
To cite this abstract in AMA style:
Bell R, Rahimi H, Lieberman A, Wood R, Schwarz E, Ritchlin C. Near Infrared Indocyanine Green Imaging Reveals Altered Anatomy and Diminished Function in Lymphatic Vessels in the Hands of Rheumatoid Arthritis Patients During Flare [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/near-infrared-indocyanine-green-imaging-reveals-altered-anatomy-and-diminished-function-in-lymphatic-vessels-in-the-hands-of-rheumatoid-arthritis-patients-during-flare/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/near-infrared-indocyanine-green-imaging-reveals-altered-anatomy-and-diminished-function-in-lymphatic-vessels-in-the-hands-of-rheumatoid-arthritis-patients-during-flare/