Session Information
Date: Sunday, November 8, 2020
Title: Epidemiology & Public Health Poster III: Inflammatory Rheumatic Disease
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: It is estimated that over 120,000 individuals currently have rheumatoid arthritis (RA) in Canada, yet a comprehensive study summarizing the epidemiology of RA burden in the country is lacking. We used data from the Global Burden of Diseases, Injuries, and Risk Factors (GBD) Study 2017 to evaluate the level, and trends over time, of disease burden indicators prevalence, mortality, years of life lost (YLLs), years lived with disability (YLDs), and disability adjusted life years (DALYs) for RA in Canada by age, sex, and socio-demographic index (SDI), from 1990 to 2017.
Methods: We obtained publicly available data from GBD Study 2017 from the Institute for Health Metrics and Evaluation interactive visualization tool (http://vizhub.healthdata.org/gbd-compare). Estimates were calculated as non-age standardized and age standardized rates per 100,000 population. GBD estimated mortality and prevalence rates based on published literature, survey data, patient records, and health insurance claims. YLLs measure years lost due to premature death calculated as the number of deaths multiplied by the standard life expectancy at each age. YLDs measure the amount of time in a year an individual lives with a short- or long-term health condition, calculated by multiplying RA prevalence with disability weights for that condition, for each age, sex, and year. DALYs was calculated as the sum of YLLs and YLDs for each age group, sex, and year. SDI combines income per capita, average educational attainment, and fertility rates. Canadian DALYs were compared to DALYs of countries with similar SDI values. All extracted data was analysed by DisMod-MR 2.1, a Bayesian meta-regression tool. All Canadian estimates were compared to global estimates.
Results: Time trends were evaluated over the study period 1990-2017. In Canada, the prevalence rate of RA increased by 55%, mortality rate decreased by 22%, YLL rate decreased by 29%, YLD rate increased by 54%, and DALY rate increased by 26%, all age-standardized. The age-standardized prevalence, mortality, YLL, YLD and DALY rates were higher in females. The Canadian prevalence rate increased at a greater rate than the global prevalence rate. The Canadian age-standardized mortality and YLL rates significantly declined after the year 2002. The global age-standardized mortality and YLLs rates declined at a slower rate than Canada. The DALY rate peaked at 70-74 and 75-78 age groups for both females and males. In 2017, YLDs contributed to 81% of the proportion of DALYs. Canada had lower age-standardized DALYs than countries of similar SDI. A weak association was found between age-standardized DALYs and SDI.
Conclusion: RA is a major public health challenge. The age-standardized prevalence, YLDs, and DALYs are increasing while mortality and YLLs are decreasing. Canada fairs better than other high SDI countries with regards to national RA burden. Early identification and management of RA is crucial to reducing the overall burden of RA in Canada, especially in women, who experience a higher burden of disease. Greater availability of data from multiple provincial RA databases would increase the accuracy and generalizability of our estimates for Canada.
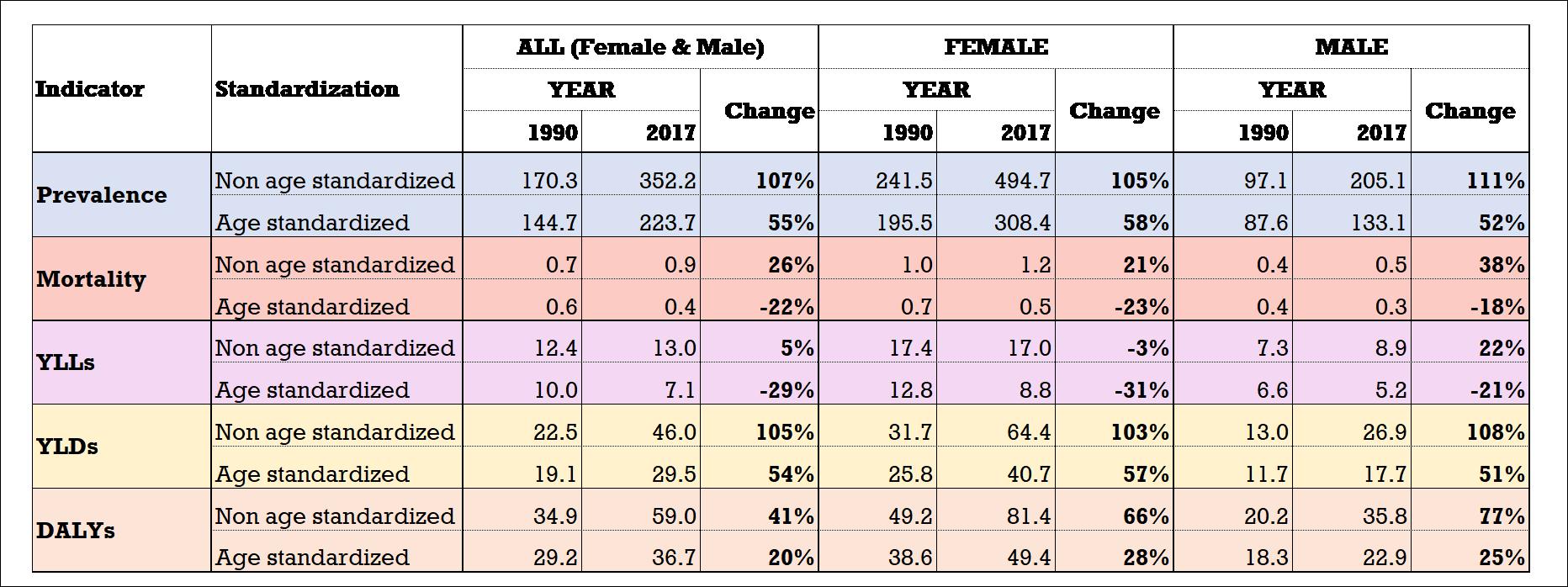 Table 1. Time Trends for Non Age Standardized and Age Standardized RA Burden of Disease Indicators per 100,000, Canada, 1990-2017
Table 1. Time Trends for Non Age Standardized and Age Standardized RA Burden of Disease Indicators per 100,000, Canada, 1990-2017
To cite this abstract in AMA style:
Hassen N, Lacaille D, Sarrafzadegan N, Xu A, Sidi S, Alandejani A, Mansourian M, Kopec J. National Burden of RA in Canada 1990-2017: Findings from the Global Burden of Disease Study 2017 [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/national-burden-of-ra-in-canada-1990-2017-findings-from-the-global-burden-of-disease-study-2017/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/national-burden-of-ra-in-canada-1990-2017-findings-from-the-global-burden-of-disease-study-2017/