Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Cardiac involvement is seen in approximately a fourth of patients with sarcoidosis, a non-necrotizing granulomatous systemic disease. Among these patients, 25% may have isolated cardiac sarcoidosis (iCS), which is now recognized as distinct phenotype. Patients usually present with heart failure (HF), ventricular arrhythmias (VA) or atrioventricular block (AVB) and have worse outcomes compared to those with systemic sarcoidosis. Given known side effects with long term glucocorticoids (GC), the conventional modality of treatment, there is an increasing role for steroid sparing agents (SSA) like mycophenolate mofetil (MMF) in iCS treatment. Most of the published experience with such agents are limited to cardiac sarcoidosis (CS), while data on the management and outcomes of iCS patients specifically, are still lacking. In our study, we aimed to characterize a cohort of iCS patients to assess their clinical and radiologic outcomes in response to treatment with MMF.
Methods: We conducted a retrospective chart review of adult patients, seen between January 2021 and January 2022, who were diagnosed with CS and were on MMF. Of these patients, those with iCS as per Japanese Circulation Society guidelines on Diagnosis and Treatment of Cardiac Sarcoidosis (2016) were included in our study. Clinical outcomes assessed included symptomatic worsening of HF, occurrence of new VA or AVB, need for left ventricular assist device (LVAD), heart transplant (HT) or death. Radiologic outcomes were based on the change in myocardial uptake on PET scans and left ventricular ejection fraction (EF) on echocardiogram after treatment with MMF. Statistical analyses were performed using Microsoft Excel.
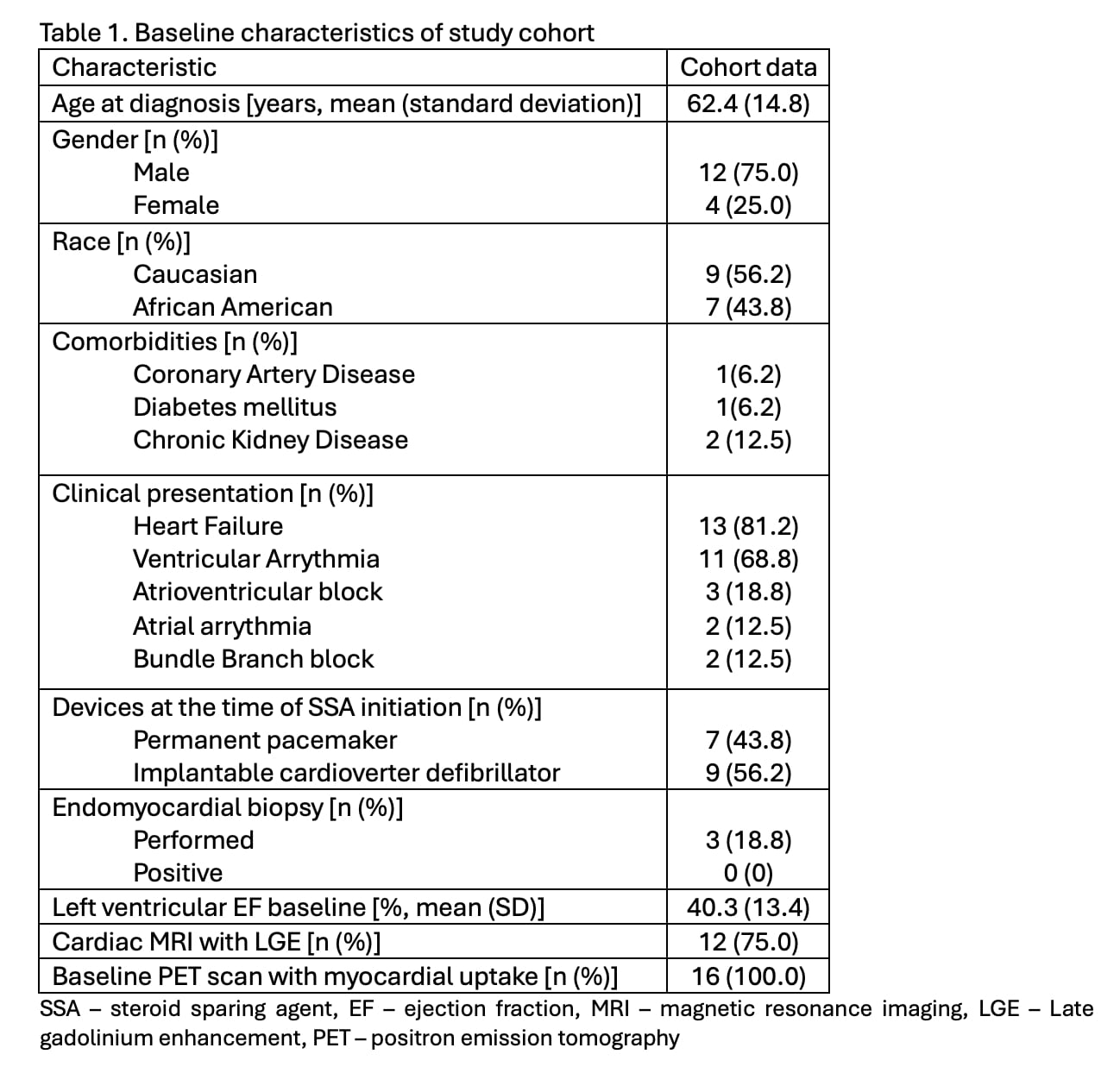
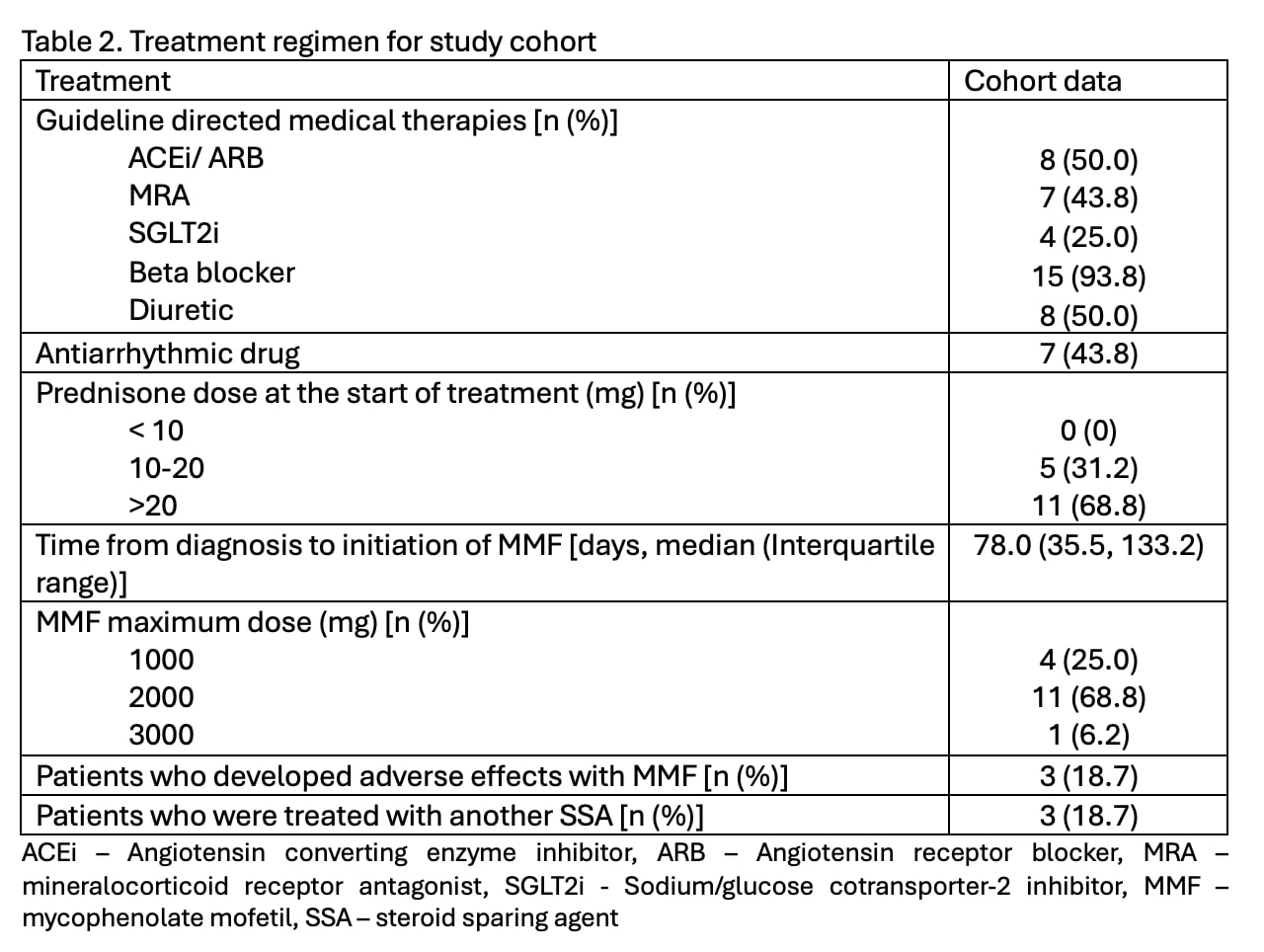
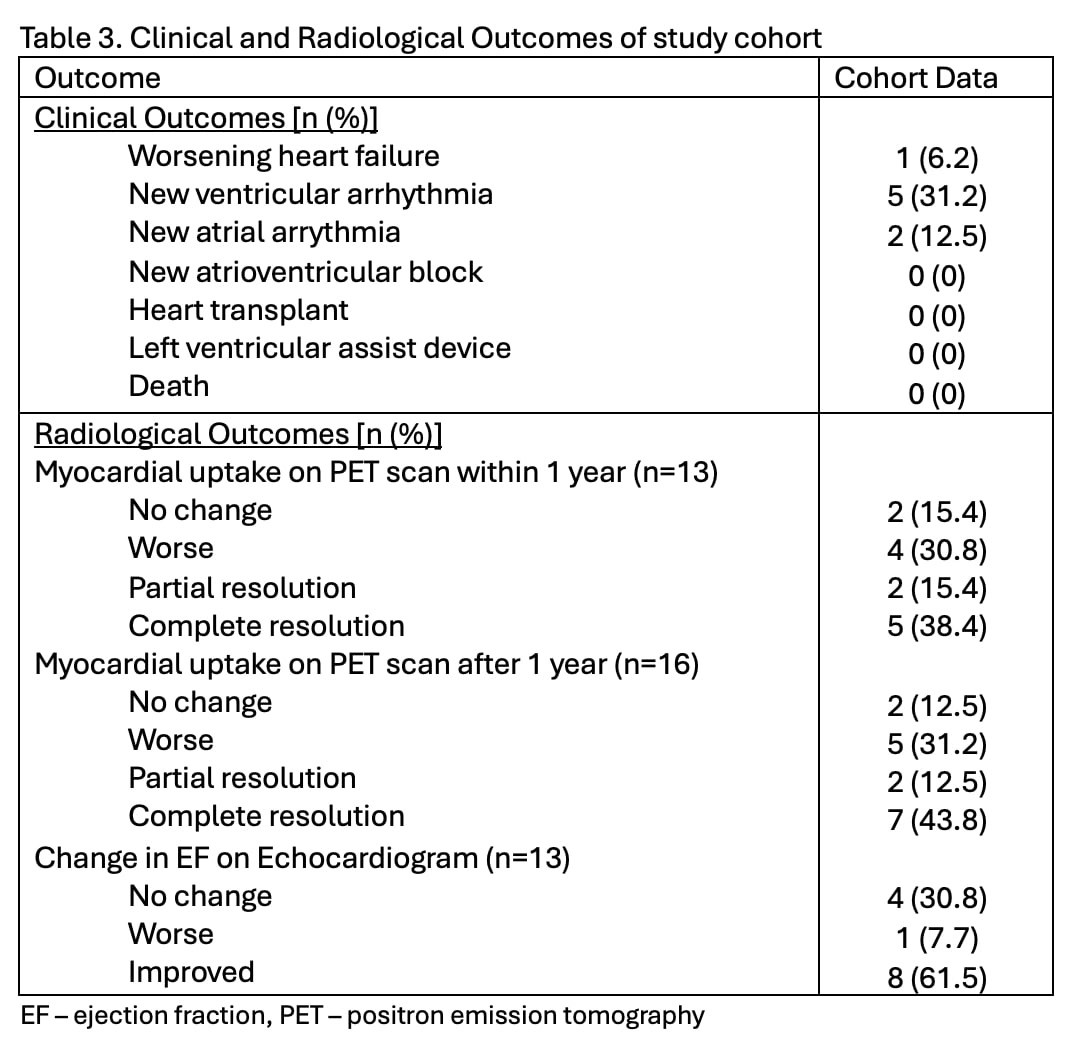
Results: Out of a total of 36 patient charts reviewed, 16 (44.4%) patients met criteria for iCS and served as our cohort. The demographics and clinical presentation are detailed in Table 1. Patients were treated with GC and then MMF as the first SSA as in Table 2. Only 3 (18.7%) patients developed adverse effects with MMF and were treated with another SSA. One (6.2%) and 5 (31.2%) patients had worsening HF and VA respectively, while no patient required LVAD, HT or died. Partial or complete cardiac resolution on PET scans within and after 1 year of diagnosis were seen in 7 (53.8%) and 9 (56.3%) patients respectively. Only 1 (7.7%) patient had worsening EF on follow up echocardiogram.
Conclusion: Though the true prevalence of iCS is hard to predict due to the variable presentation and diagnostic challenge, our study shows an iCS prevalence of 44.4% among CS patients, which is higher than the 25% reported in literature, reflecting an under-reported prevalence. Our study patients mostly presented with HF or VA, emphasizing the need for early treatment initiation. To our knowledge, this is the first study to explore MMF as an SSA in iCS treatment. Our patients were treated with a combination of GC and MMF, which was generally well tolerated and resulted in radiologic improvement in most patients. This study demonstrates the feasibility and possible efficacy of MMF in the management of iCS. Further large-scale clinical studies are required to characterize iCS and optimize treatment regimens, to reduce the morbidity and mortality linked to this rare disease.
To cite this abstract in AMA style:
Nair N, Al Saleh L, Haddad H, Jaimes Reyes M, Chetram V, Sheikh F, CONSTANTINESCU F, Pillarisetty A. Mycophenolate Mofetil in the Treatment of Patients with Isolated Cardiac Sarcoidosis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/mycophenolate-mofetil-in-the-treatment-of-patients-with-isolated-cardiac-sarcoidosis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/mycophenolate-mofetil-in-the-treatment-of-patients-with-isolated-cardiac-sarcoidosis/