Session Information
Date: Sunday, November 7, 2021
Title: RA – Diagnosis, Manifestations, & Outcomes Poster II: Miscellaneous Aspects of RA (0786–0812)
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: Treatment of rheumatoid arthritis (RA) has been advanced considerably by biological agents with capacity for stringent control of inflammation. A “treat-to-target” directive toward remission or low disease activity according to a quantitative index such as DAS28 (disease activity score), SDAI (simplified disease activity index), CDAI (clinical disease activity index), or RAPID3 (routine assessment of patient index data), is widely advocated, although it is recognized that the target must be adjusted in certain patients. The status of patients according to these indices in data from routine care has not been studied extensively and is analyzed here.
Methods: A PubMed search was conducted for “DAS28 categories – not trial,” and for “CDAI” or “RAPID3” in lieu of DAS28 in separate searches. Many reports included several indices; if SDAI also was reported, it was included in analyses. Abstracts, reports of diseases other than RA, those that did not include index data or were restricted to subsets (e.g., elderly RA patients), were excluded. No further searches were done, with a goal to provide a general overview and not a comprehensive review. Means and medians of DAS28, CDAI, RAPID3 or SDAI were analyzed in cross-tabulations. The proportions of patients in 4 index categories – high, moderate, low, and remission – was analyzed in deciles.
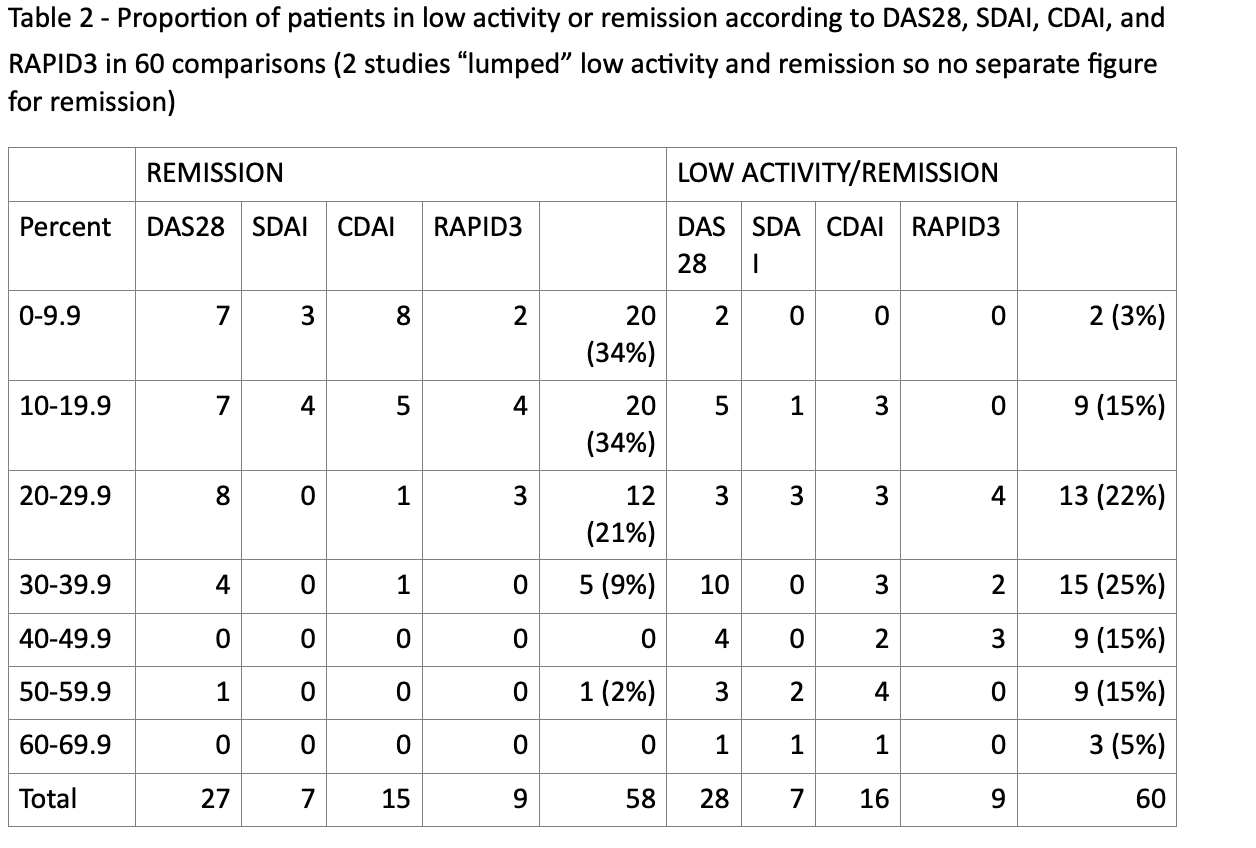
Results: A total of 51 reports met inclusion criteria, including 1, 2, 3, or 4 indices; 43 reports presented only mean or median index values, 29 reports only different categories of index activity/severity, and 22 presented both types of data. In 79 available comparisons (including several indices in many studies), 18 for CDAI, 39 for DAS28, 13 for RAPID3, and 9 for SDAI, mean or median values indicated activity/severity that was high in 16 (20%), moderate in 55 (70%), low in 8 (10%), remission in none (Table 1). Similar results were seen for the 4 indices, with 56 -77% in moderate and 13-30% in high activity/severity (Table 1). In 60 available analyses of 4 categories of activity/severity (Table 2), remission was reported in 20% or more patients in 18/58 (31%) studies, 47%, 0%, 13%, and 33% for DAS28, SDAI, CDAI, and RAPID3, respectively. Low activity/remission was reported in 40% or more patients in 21/60 (35%) studies, 25%, 43%, 44%, and 33% for DAS28, SDAI, CDAI, and RAPID3, respectively (Table 2). Mean disease duration in all studies was 7.7 years. No differences were seen according to disease duration, or any trend toward better results between 2008 and 2021.
Conclusion: The findings indicate a considerable advance over historical results in RA treatment. Nonetheless, most patients were in moderate rather than low activity/severity or remission. This study is limited by a small number of reports, many from socioeconomically disadvantaged countries, some patients in remission may be seen rarely and not be included, and higher index scores may result from comorbid fibromyalgia and/or secondary osteoarthritis and other comorbidities. Nonetheless, the results may suggest a need for changes in treatment practices, such as strategies to see patients at shorter intervals after onset of symptoms, in addition to new agents, for optimal RA treatment.

To cite this abstract in AMA style:
Schmukler J, Schroeder K, Pincus T. Most Rheumatoid Arthritis (RA) Patients from Routine Care Reported in 2008-2021 Have Improved Outcomes vs Earlier Eras, but Most Remain in Moderate/high Disease Activity Rather Than Low Activity/remission: Are New Strategies for Earlier Treatment Needed in Addition to New Agents? [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/most-rheumatoid-arthritis-ra-patients-from-routine-care-reported-in-2008-2021-have-improved-outcomes-vs-earlier-eras-but-most-remain-in-moderate-high-disease-activity-rather-than-low-activity-remis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/most-rheumatoid-arthritis-ra-patients-from-routine-care-reported-in-2008-2021-have-improved-outcomes-vs-earlier-eras-but-most-remain-in-moderate-high-disease-activity-rather-than-low-activity-remis/