Session Information
Date: Saturday, November 12, 2022
Title: RA – Treatment Poster I
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Increased risk of malignancies has been associated with chronic inflammation, as well as immunosuppressive and immunomodulatory therapies. The objective of this analysis is to describe events of malignancy in patients with rheumatoid arthritis (RA), psoriatic arthritis (PsA), or ankylosing spondylitis (AS) from the SELECT clinical trial programs for upadacitinib (UPA), a Janus kinase inhibitor, versus active comparators (adalimumab 40 mg [ADA] and methotrexate [MTX]).
Methods: Safety data (cut-off: 30 June 2021) from 9 phase 3 UPA trials were compiled for RA (6 trials), PsA (2 trials), and AS (1 trial; phase 2b/3). Treatment-emergent adverse events (TEAEs; onset on or after first dose and ≤30 days after last dose for UPA 15 mg [approved dose for rheumatological indications] and MTX or ≤70 days after last dose for ADA) of malignancy were summarized for RA (pooled UPA15, ADA [SELECT-COMPARE study only], and MTX [SELECT-EARLY study only]), PsA (pooled UPA15 and ADA [SELECT-PsA 1 study only]), and AS (UPA15). TEAEs are reported as exposure-adjusted event rates (EAERs; events/100 patient years [E/100 PY]). Age-gender adjusted standard incidence ratios (SIR) were calculated for RA, due to a sufficient number of reports, using the SEER database for the general population. Univariable Cox proportional hazards regression models were used to assess the impact of known risk factors on rates of malignancy excluding non-melanoma skin cancer (NMSC) in RA and PsA in the UPA15 treatment groups.
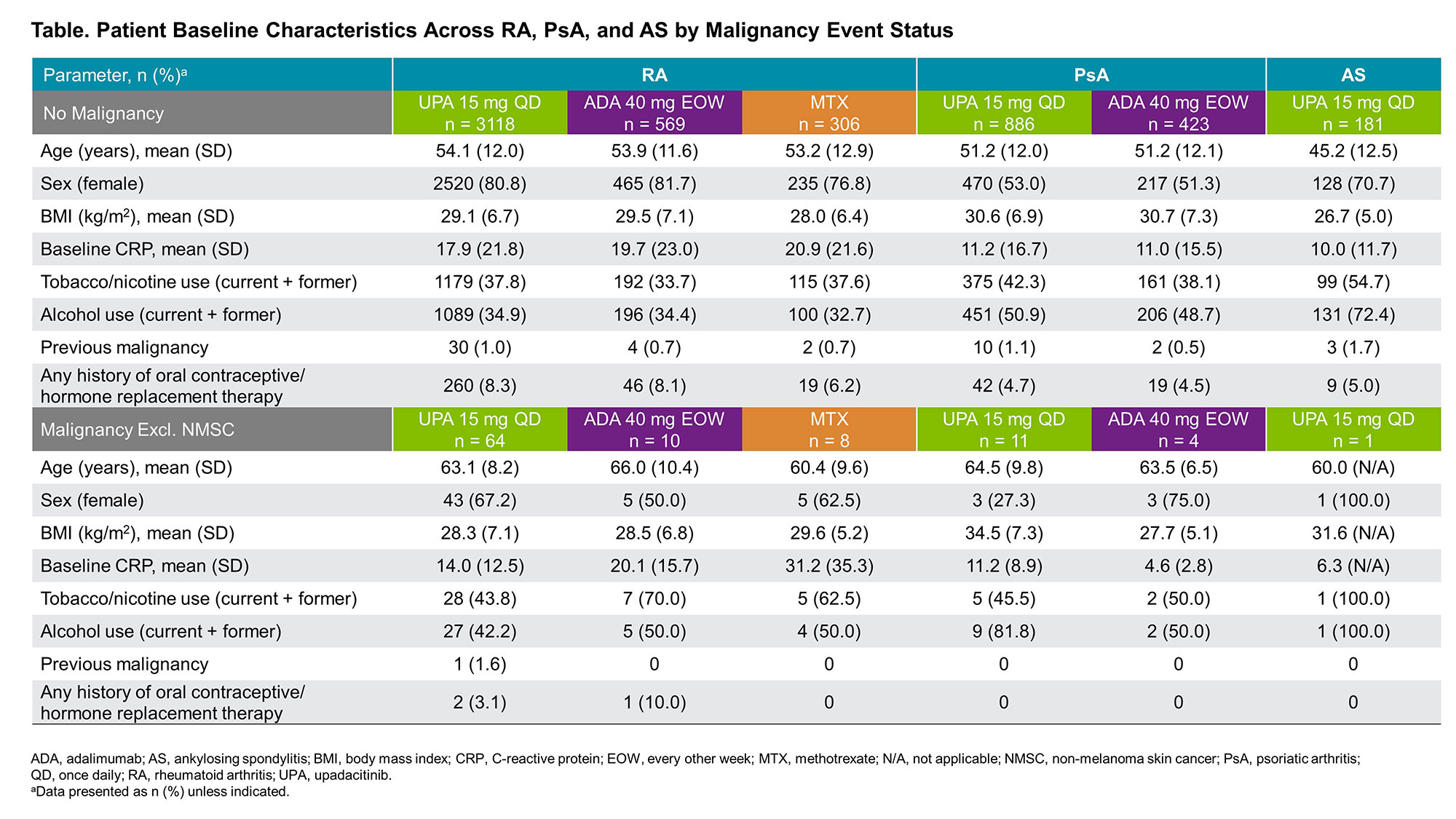
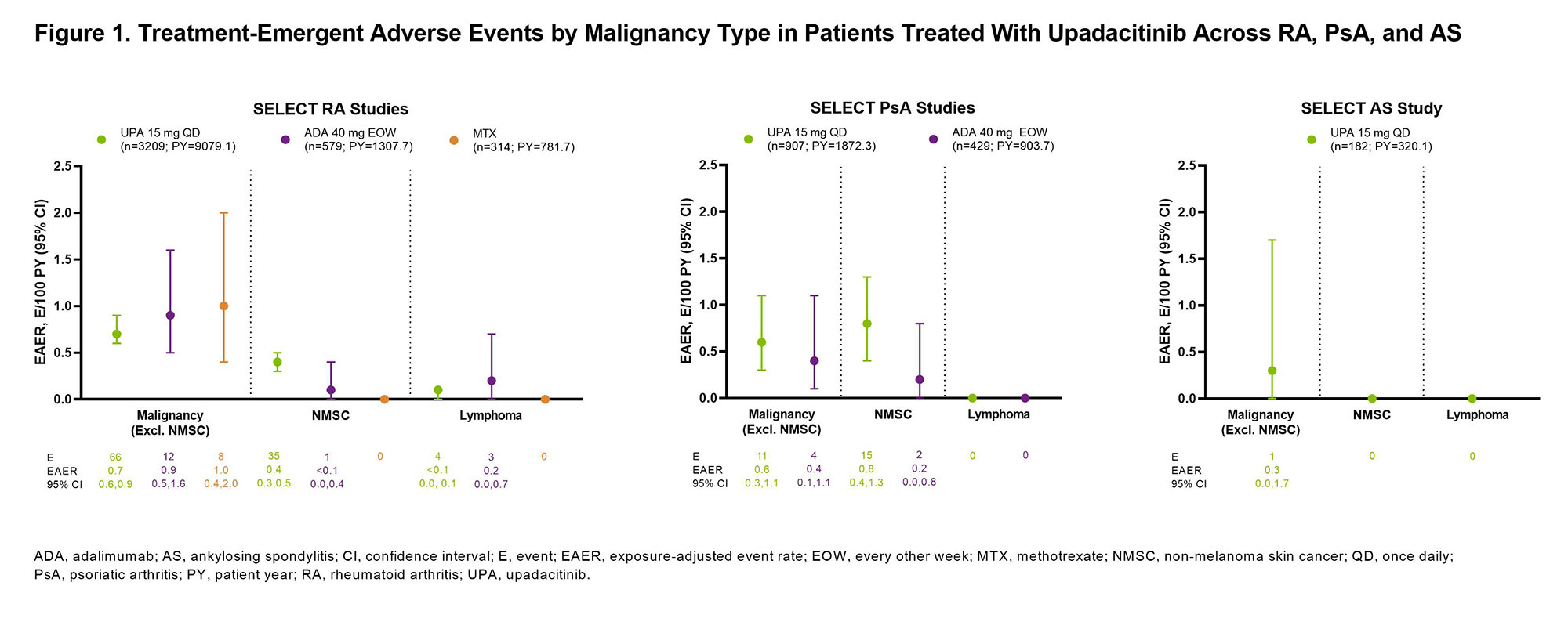
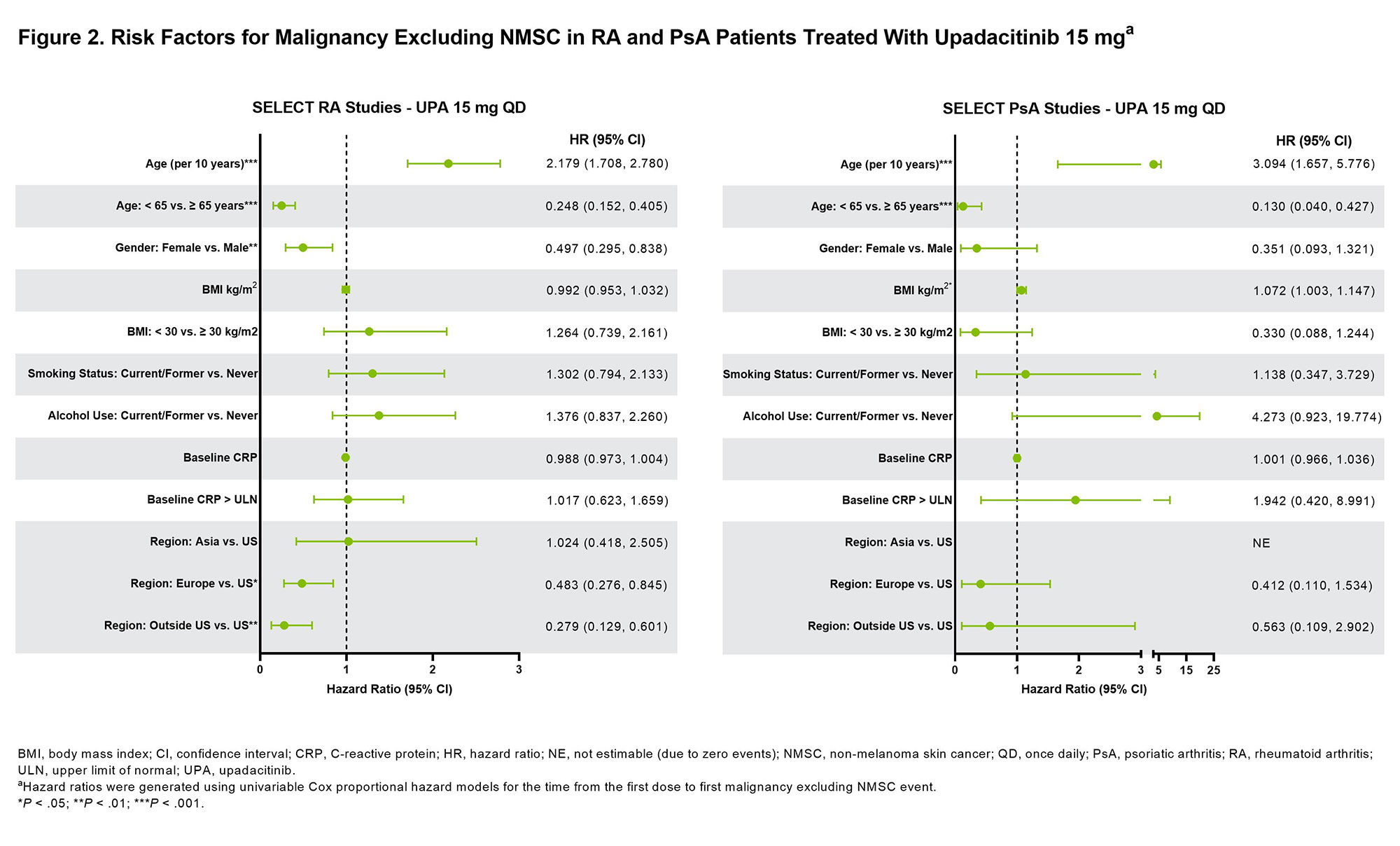
Results: Across RA, PsA, and AS, a total of 4298 patients received ≥1 dose of UPA15 (RA, n=3209; PsA, n=907; AS, n=182), totaling 11,271.5 PY of exposure (Figure 1; baseline characteristics provided in Table 1). In RA, event rates of malignancy excluding NMSC were similar between UPA15, ADA, and MTX; rates of NMSC were higher with UPA15 compared to ADA and MTX (Figure 1). The most common types of malignancy excluding NMSC were breast cancer and lung cancer. The age-gender adjusted SIR (95% CI) for malignancy excluding NMSC in RA was 1.0 (0.80-1.24) for UPA15. In PsA, rates of NMSC and malignancy excluding NMSC were similar between UPA15 and ADA. In AS, a single event of malignancy excluding NMSC was reported with UPA15. Lymphoma was infrequent in RA, with no events in PsA or AS. In the univariable regression models for UPA15, being older, male, and in the US compared to other regions were associated with increased risk of malignancy excluding NMSC in patients with RA, while being older and having higher BMI were associated with increased risk in patients with PsA (Figure 2).
Conclusion: Event rates of malignancy excluding NMSC were generally similar between UPA15, ADA, and MTX and consistent across RA, PsA, and AS. NMSC was more frequent in patients receiving UPA15 than ADA or MTX. Due to low rates of malignancy, findings from the univariable regression models will need to be confirmed in future studies.
To cite this abstract in AMA style:
Rubbert-Roth A, Kakehasi A, Takeuchi T, Schmalzing M, Palac H, Liu J, Anyanwu S, Lippe R, Curtis J. Malignancy in the Upadacitinib Clinical Trial Programs for Rheumatoid Arthritis, Psoriatic Arthritis, and Ankylosing Spondylitis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/malignancy-in-the-upadacitinib-clinical-trial-programs-for-rheumatoid-arthritis-psoriatic-arthritis-and-ankylosing-spondylitis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/malignancy-in-the-upadacitinib-clinical-trial-programs-for-rheumatoid-arthritis-psoriatic-arthritis-and-ankylosing-spondylitis/