Session Information
Date: Sunday, October 21, 2018
Title: Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster I: Comorbidities
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Early atherosclerotic lesions appear as non-calcified plaques (NCP) on a non-invasive coronary artery evaluation by computed tomography angiography (CCTA). Advanced, more vulnerable lesions appear as mixed/ partially calcified plaques (MP) or calcified plaques (CP). We evaluated the role of inflammation, medication exposure and cardiac risk factors (CRFs) on NCP generation and progression in RA patients with a follow-up evaluation of coronary anatomy with CCTA.
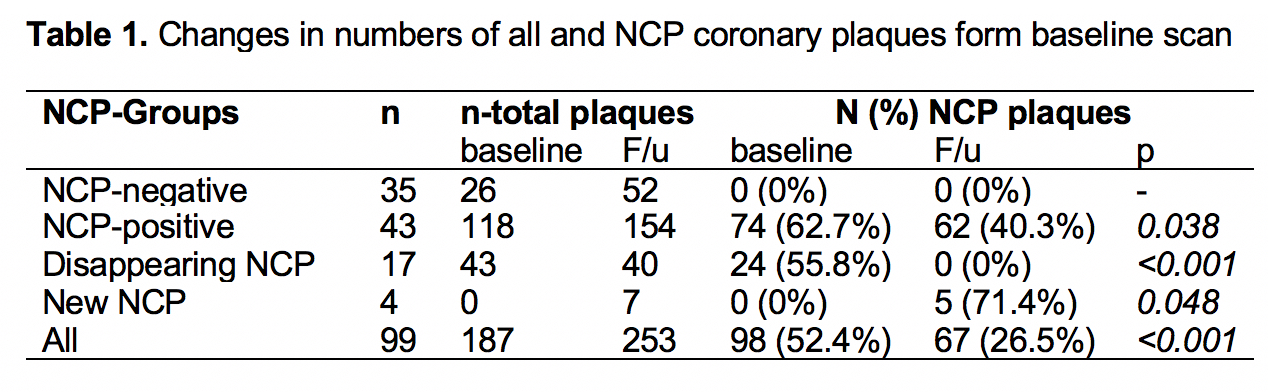
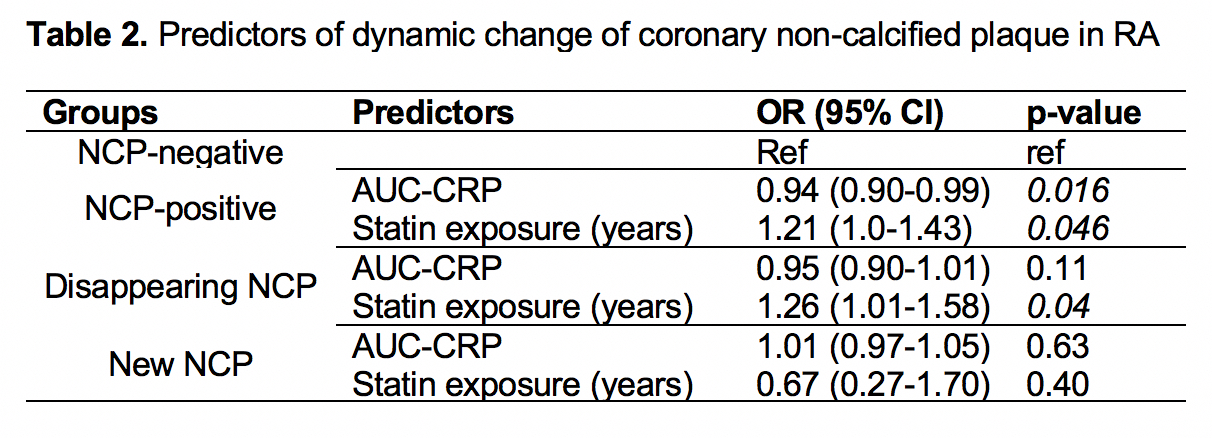
Methods: Ninety-nine participants underwent a repeat CCTA assessment within 83±3.6 months. All coronary lesions were counted and characterized as NCP, MP, or CP; prevalence, number, stenotic severity and burden of individual NCP plaques on both baseline and follow-up scans was recorded. Patients were subsequently classified into four groups according to plaque disposition: NCP-negative (no NCP at any time), NCP-positive (NCP present at both times), disappearing-NCP (present at baseline, absent at follow-up), or new-NCP (absent at baseline, present at follow-up). A Multinomial logistic regression model evaluated predictors independently associated with classification of patients into the respective NCP groups compared to the NCP-negative group.
Results: Overall NCP prevalence was lower at follow-up compared to the baseline assessment (26.5% vs. 52.4%, p<0.001, table 1); 21 of 99 (21%) patients showed disappearance or development of new NCP lesions. In the NCP-positive group, 68% of the follow-up NCP plaques derived from original NCP lesions, with the vast majority (93%) displaying identical stenotic severity and burden; 29% were incident NCP plaques. Of baseline NCP lesions, 18% receded. In the disappearing group, 75% of the original NCP plaques receded, whereas 16% transitioned to more stable calcified plaques (CP). Patients in the NCP-positive group displayed lower cumulative inflammatory burden [area under the curve for c-reactive protein (AUC-CRP), p=0.016] and longer duration of statin exposure compared to the NCP-negative ones (table 2, p=0.046). NCP disappearance was mostly predicted by lengthier statin exposure (p=0.04).
Conclusion: Lower inflammatory burden and longer statin exposure inhibit NCP growth or progression to more advanced, vulnerable plaques. Lengthier statin exposure may further induce regression of such early atherosclerotic lesions.
To cite this abstract in AMA style:
Karpouzas G, Ormseth S, Hernandez E, Budoff M. Low Inflammatory Burden and Statin Exposure Inhibit Progression and Induce Regression of Early Coronary Plaques in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/low-inflammatory-burden-and-statin-exposure-inhibit-progression-and-induce-regression-of-early-coronary-plaques-in-rheumatoid-arthritis/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/low-inflammatory-burden-and-statin-exposure-inhibit-progression-and-induce-regression-of-early-coronary-plaques-in-rheumatoid-arthritis/