Session Information
Date: Sunday, November 7, 2021
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: Bone marrow edema (BME) and erosions of the sacroiliac (SI) joints are key imaging features in the diagnosis of axial spondyloarthritis (axSpA). MRI with a fluid sensitive sequence is the most common technique for confirming BME but disadvantages include cost and accessibility. Traditional CT is considered superior for detection of erosions but may be limited by radiation exposure. Low dose CT is a technique associated with a similar amount of radiation as conventional radiography and low dose dual energy CT (ldDECT) may be able to detect BME without the need for higher doses of radiation.
We aim to compare the ability of ldDECT and MRI STIR for the detection of BME and erosions of the SI joints in an inception cohort of patients presenting with undiagnosed back pain and psoriasis, iritis, colitis, or positive HLA-B27.
Methods: Consecutive patients ≤ 45 years of age with ≥ 3 months of undiagnosed low back or buttock pain with any one of psoriasis, uveitis, inflammatory bowel disease, or positive HLA-B27 underwent routine clinical evaluation by a rheumatologist for axSpA followed by both MRI and ldDECT of the SI joints done within 3 months of each other.
Two musculoskeletal fellowship trained radiologists were given 17 cases for calibration which were not included in the study. MRI images were scored for presence of BME, presence of large BME lesions, erosions, number of erosions, and radiologist global assessment for presence/absence of sacroiliitis with confidence scale (0-10) blinded to clinical information and ldDECT images. ldDECT images were scored in the same manner and discordant reads were adjudicated by a third radiologist.
Results: 68 patients were recruited with 27 (39.7%) diagnosed with axSpA (mean age 33.2, male 63%, mean symptom duration 8.7 years, HLA-B27 positive 85%). Uveritis, psoriasis, and IBD were present in 20, 23, and 6% of patients respectively.
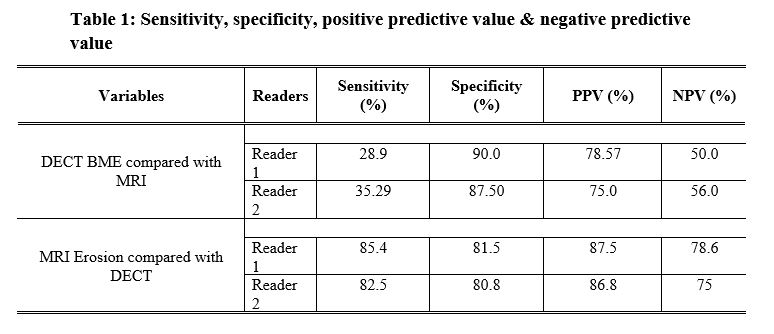
ldDECT had a sensitivity of 28.9 and 35.3% and a specificity of 90 and 87.5% between two readers for detection of BME compared with MRI (Table 1).
MRI had a sensitivity of 85 and 82.5% and a specificity of 81.5 and 80.8% between two readers for detection of erosions compared with ldDECT.
Inter-reader reliability was higher for MRI detected BME and erosions compared with DECT (Table 2).
Amongst patients who were diagnosed by a rheumatologist as having axSpA (n=27), 21 had sacroiliitis seen on both CT and MRI, 2 only on CT, 1 only on MRI, and 3 on neither.
Conclusion: ldDECT displayed a reduced sensitivity but was highly specific for BME compared to MRI STIR sequence as a reference standard. MRI revealed reasonable sensitivity and specificity for erosions compared to ldDECT as a reference standard. ldDECT has good reproducibility for the interpretation of erosions but has moderate inter-reader reliability for BME.
Amongst patients where BME was detected, 86% had evidence of erosive changes suggesting a marginal benefit with addition of dual energy scanning. Only 1 patient eventually diagnosed with axSpA had sacroiliitis on MRI not seen on ldDECT. Given the potential lower cost and accessibility of ldDECT, further studies may reveal whether utilizing ldDECT as the initial imaging modality would reduce the need for an MRI and thus increase accessibility and reduce costs.

To cite this abstract in AMA style:
Chan J, Nicolaou S, Yan Y, Osman M, Ouellette H, Jalal S. Low Dose Dual Energy CT Scan for the Detection of Bone Marrow Edema and Erosions in Axial Spondyloarthritis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/low-dose-dual-energy-ct-scan-for-the-detection-of-bone-marrow-edema-and-erosions-in-axial-spondyloarthritis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/low-dose-dual-energy-ct-scan-for-the-detection-of-bone-marrow-edema-and-erosions-in-axial-spondyloarthritis/