Session Information
Date: Monday, October 27, 2025
Title: (1467–1516) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Anti-dsDNA antibodies are a key diagnostic marker of systemic lupus erythematosus (SLE), often associated with active disease. Its presence is detected using various commercial assays including enzyme-linked immunosorbent assay (EIA), multiplexed flow immune assay (MFIA) and the Crithidia lucilae immunofluorescence assay (CLIFT), which differ in sensitivity, specificity and methodology. This variability complicates interpretation of anti-dsDNA results in relation to disease activity. Using a multiethnic, longitudinal SLE cohort, the analysis compares anti-dsDNA measurements by CLIFT, EIA and MFIA with disease activity.
Methods: Patients with SLE from Bellevue Hospital Center were included. All patients fulfilled SLE criteria by at least one method: American College of Rheumatology (ACR), Systemic Lupus Erythematosus International Collaborating Clinics (SLICC) and/or 2019 ACR/European League Against Rheumatism (EULAR) classification criteria. A change in commercial anti-dsDNA antibody testing from enzyme immunoassay (EIA) to multiplex flow immunoassay (MFIA) on April 1, 2024, served as a natural point for analysis. Patients with anti-dsDNA results by EIA, CLIFT and MFIA within one year before and after this transition were identified. Titre and concordance or discordance among assays and association with ACR criteria lupus nephritis (LN) were analyzed.
Results: Of the 135 patients with SLE, 50% were Hispanic, 30% were Black, 17% were Asian, and 4% were unknown. Paired testing with EIA and CLIFT was performed in 103 patients, and MFIA and CLIFT in 104 patients. Comparison between CLIFT and EIA revealed that 57% of patients had consistently concordant results, 31% showed fluctuating concordance, and 12% were consistently discordant (Figure 1). Similarly, 60% of patients had concordant results between CLIFT and MFIA, 13% fluctuated, and 27% were consistently discordant. Following the transition from EIA to MFIA in April, 109 patients demonstrated concordant results between EIA and MFIA, while 26 had discordant findings. Among 68 patients with ACR criteria LN, 20 tested positive by EIA, 22 by MFIA and 29 by CLIFT. The specificity and sensitivity for detecting LN were 77% and 26% for EIA, 73% and 32% for MFIA, and 47% and 47% for CLIFT, respectively.
Conclusion: This cohort demonstrates that current anti-dsDNA antibody testing using CLIFT, in conjunction with EIA or MFIA shows limited concordance. Despite EIA and MFIA being similar immunoassays, 23% of patients exhibited discordant results following the laboratory decision to change assay. In our cohort, CLIFT had the lowest specificity for identifying patients with LN. Moreover, failing to identify anti-dsDNA antibody positive status by restricted method testing can have an impact on meeting SLE disease classification criteria and/or accurately determining disease activity. These findings suggest incorporating multiple dsDNA antibody assays may enhance the accuracy of SLE classification and ensure more reliable assessment of disease activity during routine monitoring.
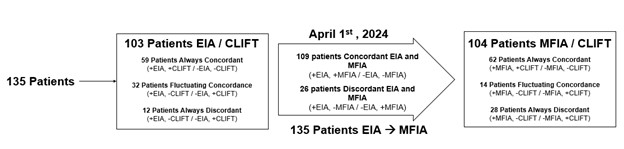 Figure 1. Flow diagram illustrating concordance and discordance of EIA and CLIFT or MFIA and CLIFT as well as the transition from EIA to MFIA immunoassays.
Figure 1. Flow diagram illustrating concordance and discordance of EIA and CLIFT or MFIA and CLIFT as well as the transition from EIA to MFIA immunoassays.
To cite this abstract in AMA style:
Dai J, Izmirly P, Buyon J, Belmont H. Limited Concordance Between anti-dsDNA Assays and Association with Lupus Nephritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/limited-concordance-between-anti-dsdna-assays-and-association-with-lupus-nephritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/limited-concordance-between-anti-dsdna-assays-and-association-with-lupus-nephritis/