Session Information
Date: Sunday, November 7, 2021
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster II: Manifestations (0855–0896)
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: Cognitive dysfunction (CD) is reported to affect approximately 40% of SLE patients (1). Mood disorders have been associated with both cognitive symptoms and cognitive function in SLE, but the associations of fibromyalgia with these are unclear. We investigated the relationships between patient-reported cognitive symptoms and objective cognitive test results in SLE, and associations of fibromyalgia and mood disorders with both.
Methods: We tested SLE patients (n=87) and demographically matched healthy control (HC) participants (n=48) with the one-hour neuropsychiatric test battery recommended by the ACR for use in SLE (2) and applied three binary definitions of CD and seven cognitive test z-scores. We assessed patient-reported cognitive symptoms, mood disorder symptoms, fibromyalgia symptoms, and fatigue using the Cognitive Symptoms Inventory (CSI), Hospital Anxiety and Depression Scale (HADS), Central Sensitivity Score (CSS) derived from the 2016 ACR fibromyalgia diagnostic criteria (3) and the Functional Assessment of Chronic Illness Therapy Fatigue Scale (FACIT), respectively. We performed multivariate regression analysis to determine associations with cognitive endpoints; likelihood ratio tests were used to select for inclusion from collinear pairs. We used unpaired t tests to compare CSI scores between groups.
Results: Among SLE patients, the median (range) age was 45 (22-64). Compared to HC, CSS scores were higher (< 0.00001), fibromyalgia was more common (p 0.009) and a history of depression or anxiety was more frequent (p< 0.0001) in SLE patients (Table 1). Cognitive symptoms (CSI score) were worse in SLE patients than HC (median (range) 33 (19-52) vs. 26.5 (21-35), p < 0.0001). At all thresholds, cognitive dysfunction was also more frequent in SLE patients than HC. Age and premorbid IQ were significantly associated with multiple cognitive test endpoints but not with CSI score. On multivariate analysis, CSS, a history of depression, and HADS Anxiety each had significant associations with at least one CD endpoint, but history of anxiety or FACIT score did not. On univariate analysis, cognitive symptoms (CSI) consistently correlated with CSS, FACIT and all mood disorder covariates (CSI) (p 0.02 - < 0.001); on multivariate analysis, after selecting from collinear pairs, only CSS remained significant (p< 0.0001) (Table 2). There were no associations between cognitive symptoms and cognitive test results. Correspondingly, there was no significant difference in cognitive symptoms (CSI score) between cognitively impaired and unimpaired SLE patients at any cognitive impairment threshold (p values 0.22-0.47).
Conclusion: Cognitive impairment, and cognitive symptoms, are each common in patients with SLE, but there were no associations between patient-reported cognitive symptoms and objective cognitive test results. Depression, anxiety and fibromyalgia were more strongly associated with cognitive symptoms than with test results. The distinction between cognitive symptoms and cognitive function needs to be considered when assessing SLE patients with CD.
References: 1) Al Rayes et al. Semin Arthritis Rheum 2018. 2) Liang et al. Arthritis Rheum 1999. 3) Wolfe et al. Semin Arthritis Rheum 2016.
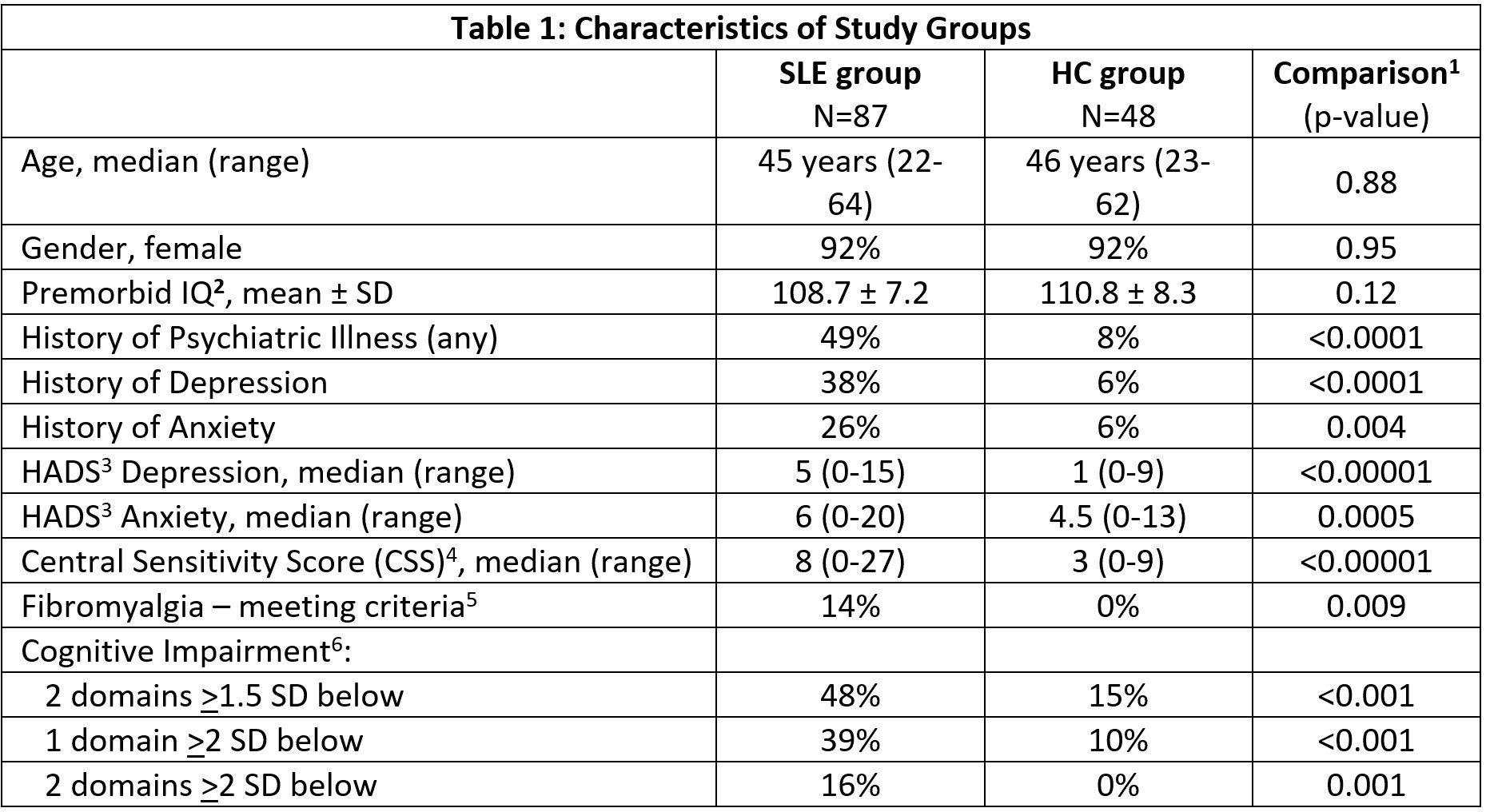
1) Sociodemographic variables were compared between the SLE and control groups using Mann-Whitney, Chi squared and T tests. 2) Premorbid IQ measured by Test of Premorbid Functioning scaled score. 3) HADs – Hospital Anxiety and Depression Scale. 4) Central Sensitivity Score = Widespread Pain Index plus Symptom Severity Score as per 2016 ACR Fibromyalgia Diagnostic Criteria. 5) Meeting 2016 ACR Fibromyalgia Diagnostic Criteria. 6) Impairment defined by number of cognitive domains either 1.5 or 2 standard deviations (SD) below healthy control group mean.
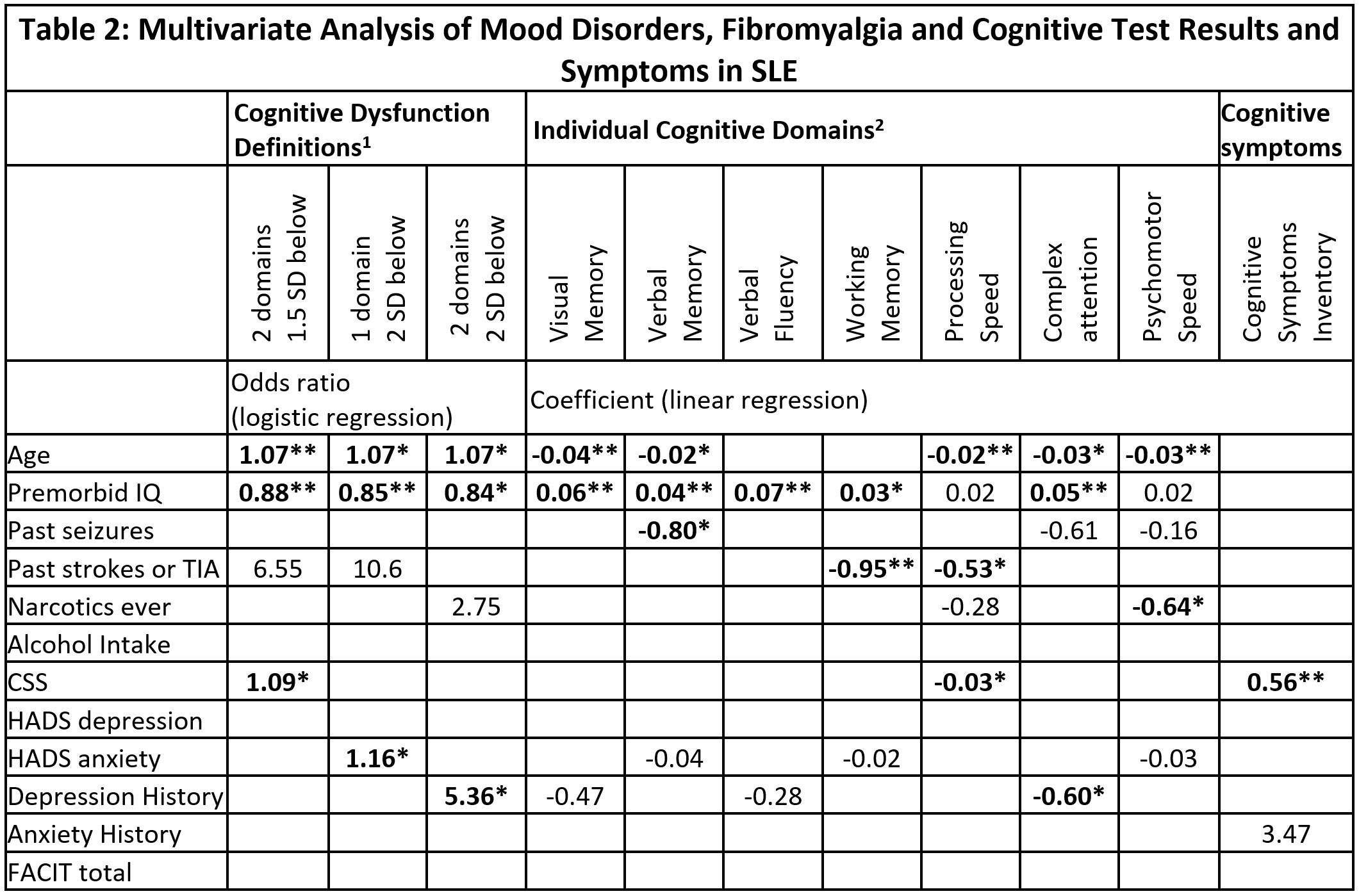
Significant results bolded: *p value <0.05 **p value <0.005.
1) Impairment defined by number of cognitive domains either 1.5 or 2 SD below healthy control group mean. 2) Specific cognitive tests used for each domain are as follows: Visual Memory – Rey Ostrrieth Complex Figure Test Recall Score, Verbal Memory -California Verbal Learning Test trials 1-5, Verbal Fluency – Controlled Oral Word Association Test FAS Sum, Working Memory – Letter Number Sequencing score, Processing Speed – Coding score, Complex Attention – Trail making test B time inverse, Psychomotor speed – finger tap test dominant hand score. 3) for FACIT scores higher scores represent less fatigue (better functioning). Acronyms: TIA – transient ischaemic attack, CSS – Central Sensitivity Score derived from 2016 Fibromyalgia diagnostic criteria, HADS – Hospital Anxiety and Depression Scale, FACIT – Functional Assessment of Chronic Illness Therapy Fatigue Scale. CSI – Cognitive Symptoms Inventory, SD – standard deviations.
To cite this abstract in AMA style:
Raghunath S, Glikmann-Johnston Y, Guymer E, Morand E, Stout J, Hoi A. Lack of Association Between Cognitive Test Performance and Cognitive Symptoms in Systemic Lupus Erythematosus (SLE) [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/lack-of-association-between-cognitive-test-performance-and-cognitive-symptoms-in-systemic-lupus-erythematosus-sle/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/lack-of-association-between-cognitive-test-performance-and-cognitive-symptoms-in-systemic-lupus-erythematosus-sle/