Session Information
Date: Monday, November 13, 2023
Title: (1124–1154) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients consult rheumatologists for symptoms which may result from inflammatory activity or reversible problems (INF), joint or other organ damage or irreversible problems (DAM), and/or distress with neither INF nor DAM (STR), e.g., fibromyalgia. Many patients may have clinically important DAM and/or STR in addition to INF. However, quantitative assessment in routine rheumatology care is directed primarily (often exclusively) to INF, e.g., DAS28, CDAI, SLEDAI, ASDAS, and DAPSA. DAM and STR are recognized in many patients, but generally recorded only as narrative descriptions, rather than as quantitative data. INF indices are effective in clinical trials. However, measures and indices designed to assess INF may be elevated by comorbid DAM and/or STR, often despite little or no INF, particularly in routine care patients. A RheuMetric checklist includes 4 0-10 visual numeric scales (VNS) for physician global assessment (DOCGL), inflammation (DOCINF), damage (DOCDAM), and patient distress (DOCSTR), and estimates of the percent of DOCGL attributed to INF, DAM, and STR. We analyzed RheuMetric scores in routine care patients with all diagnoses at initial or return visits to recognize levels of DOCGL, INF, DAM, and STR at initial vs follow-up visits.
Methods: A retrospective cross-sectional study was performed of RheuMetric checklist 0-10 VNS estimates for DOCGL and estimates of %INF, %DAM, and %STR (total=100%) completed in routine care by the treating rheumatologist. Mean levels of these estimates were analyzed according to primary diagnosis, classified as INF (RA, SLE, SpA, vasculitis and gout), osteoarthritis (OA), primary fibromyalgia (FM), and “other,” at initial or return visits, using descriptive and chi-square statistics.
Results: Highest DOCINF was in inflammatory diseases, DOCDAM in OA, and DOCSTR in primary FM (Table). The % of DOCGL attributed to INF, DAM, and STR was highest in INF diseases, OA, and primary FM, respectively (p< 0.001) (Table). At initial visits of patients with inflammatory diseases, mean DOCGL was 4.3, attributed 62% to INF, 24% to DAM and 14% to STR, respectively. At return visits of patients with inflammatory diseases, mean DOCGL was 3.7, attributed 33% to INF, 49% to DAM and 18% to STR (Table). In patients with all diagnoses, 36%, 36%, and 28% of DOCGL were attributed to INF, DAM, and STR, respectively, at first visits, vs 22%, 51%, and 28% at return visits (Table). RheuMetric estimates required 15-20 seconds to complete.
Conclusion: RheuMetric physician estimates for INF, DAM, and STR are feasibly recorded in 15-20 seconds in routine care, with face validity documented by significantly higher DOCINF in inflammatory diseases, DOCDAM in OA, and DOCSTR in FM. DOCINF was higher at first vs return visits, reflecting strong anti-inflammatory therapies at this time, while % DOCDAM was higher at return vs first visits. At return visits of all patients, INF accounted for 22% of DOCGL vs 50% for DAM and 28% for STR, indicating that control of inflammation is not the primary rheumatology activity after the first visit. Physician 0–10 estimates of inflammation, damage, and patient distress, in addition to DOCGL, can give a more complete quantitative patient assessment than only measures of inflammation.
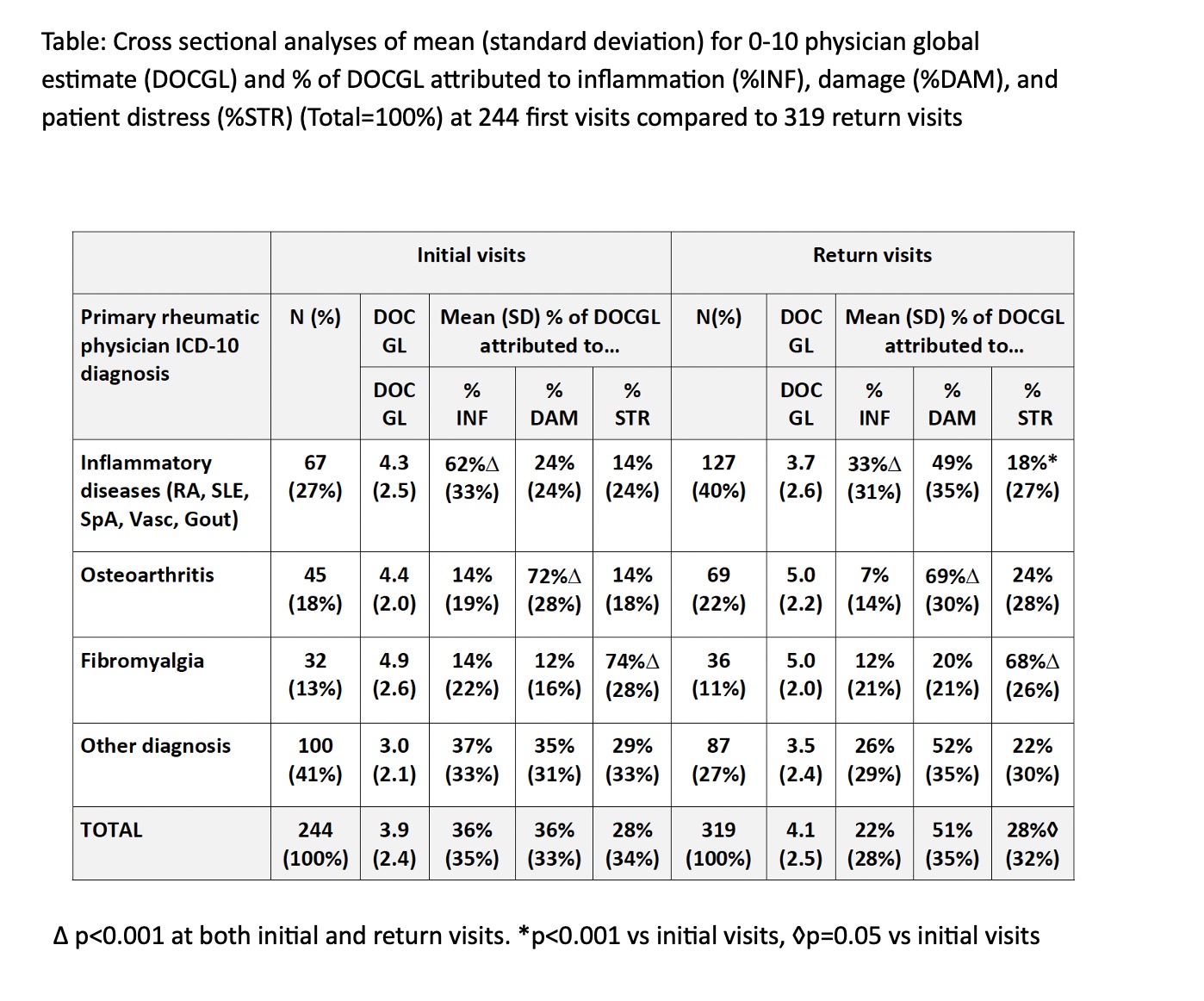
estimate (DOCGL) and % of DOCGL attributed to inflammation (%INF), damage (%DAM), and
patient distress (%STR) (Total=100%) at 244 first visits compared to 319 return visits
Δ p<0.001 at both initial and return visits. *p<0.001 vs initial visits, ◊p=0.05 vs initial visits
To cite this abstract in AMA style:
Pincus T, Li T, Schmukler J. Inflammation Is More Prominent Than Joint Damage at Initial Visits of Patients with Inflammatory Arthritides, but Organ Damage Is More Prominent and Patient Distress Is as Prominent as Inflammation in Overall Rheumatology Care: Data from a Feasible Physician RheuMetric Checklist [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/inflammation-is-more-prominent-than-joint-damage-at-initial-visits-of-patients-with-inflammatory-arthritides-but-organ-damage-is-more-prominent-and-patient-distress-is-as-prominent-as-inflammation-in/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/inflammation-is-more-prominent-than-joint-damage-at-initial-visits-of-patients-with-inflammatory-arthritides-but-organ-damage-is-more-prominent-and-patient-distress-is-as-prominent-as-inflammation-in/