Session Information
Date: Sunday, October 26, 2025
Title: (0671–0710) Systemic Sclerosis & Related Disorders – Clinical Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: The incidence of sudden cardiac death (SCD) is suspected to be increased in systemic sclerosis (SSc). However, data describing SCD incidence in SSc are sparse and confined to small cohorts. Accordingly, this study aims to estimate SCD incidence in SSc and assess the association with disease characteristics.
Methods: Individuals from the Australian Scleroderma Cohort Study with a definable SSc subtype meeting ACR/EULAR criteria were included. International Classification of Diseases (ICD)-10 code cause of death was sourced from the Australian National Death Index. Two authors adjudicated SCD events, which were considered present when an ICD-10 code cause of death for an acute cardiovascular pathology was listed (sudden cardiac death, cardiac arrest, ventricular fibrillation/flutter, acute myocardial infarction/acute ischaemic heart disease (IHD), ventricular tachycardia, cardiac tamponade, pericardial effusion, aortic or mitral valve lesion) excluding those with major pulmonary, renal or gastrointestinal primary causes of death. Between-group comparisons (SCD vs. overall cohort) were performed using Chi-squared testing or Wilcoxon rank-sum testing as appropriate, and multivariable Cox proportional hazard modelling was used to identify associations of SCD.
Results: Among 1708 SSc patients, 32 SCD events occurred (1.9%) over 10,650 person-years’ follow-up (Figure 1), equivalent to an observed incidence rate of 300 per 100,000 person-years. This rate is 3-9 times higher than published general population estimates (35-89/100,000 person-years).1,2Participants who experienced SCD were more likely to have IHD (40.6% vs. 13.8%, p < 0.001) and reduced left ventricular ejection fraction (LVEF < 50%; 18.5% vs. 5.5%, p=0.004). SSc heart involvement (18.8% vs. 9.4%, p=0.074), aortic valve pathology (12.9% vs. 5.7%, p=0.089) and pulmonary hypertension (18.8% vs. 11.3%, p=0.188) were numerically more common in those with SCD, although not meeting statistical significance. While cardiovascular risk factors including hypertension, dyslipidaemia and smoking history were not associated with SCD, these patients were numerically more likely to have two or more of these factors (60.7% vs. 47.5%, p=0.165). Multivariable Cox hazard modelling identified that older age (hazard ratio (HR) 1.15 (95% confidence interval (CI) 1.10-1.20), p < 0.001), IHD (HR 2.28 (95%CI 1.04-5.00), p=0.040), reduced LVEF (HR 2.89 (95%CI 1.06-7.90), p=0.038) and smoking exposure (HR 2.80 (95%CI 1.21-6.49), p=0.016) were associated with SCD.
Conclusion: SCD occurred in 1.9% of a large SSc cohort, with an incidence rate of 300 per 100,000 person-years. This is significantly higher than the rate of SCD reported in the general population. Older age, IHD, reduced LVEF and smoking were key risk factors for SCD, highlighting important and potentially modifiable risk factors for SCD in SSc. References1. Wong CX, Brown A, Lau DH, et al. Epidemiology of Sudden Cardiac Death: Global and Regional Perspectives. Heart Lung Circ 2019; 28(1): 6-14.2. Empana JP, Lerner I, Valentin E, et al. Incidence of Sudden Cardiac Death in the European Union. J Am Coll Cardiol 2022; 79(18): 1818-27
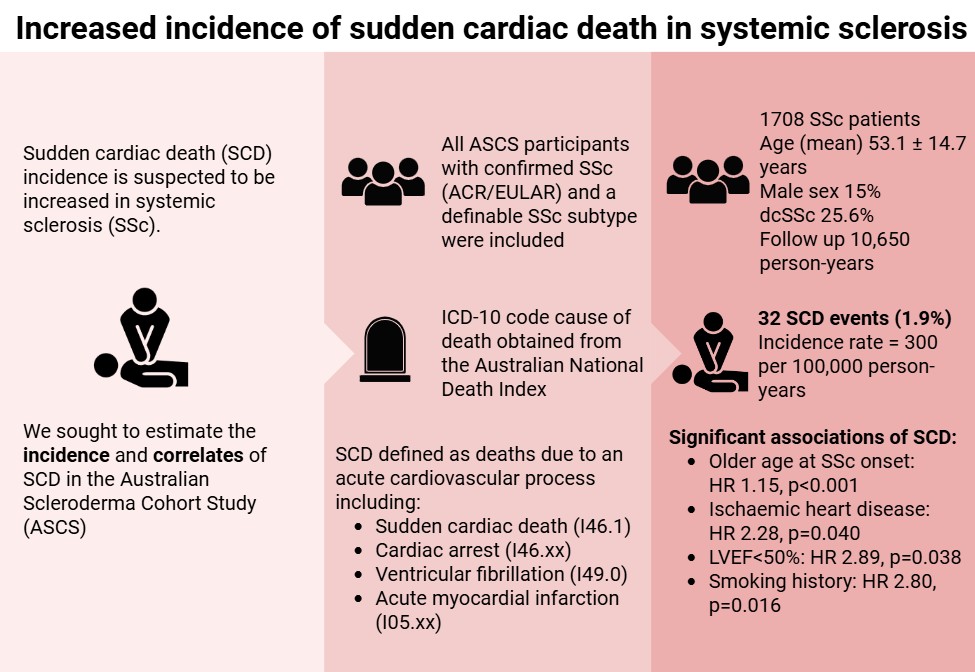 Figure 1: Graphical Abstract
Figure 1: Graphical Abstract
To cite this abstract in AMA style:
Fairley J, Paratz E, Hansen D, Proudman S, Sahhar J, Ngian G, Apostolopoulos D, Walker J, Host L, Stevens W, La Gerche A, Nikpour M, Ross L. Increased incidence of sudden cardiac death in systemic sclerosis: estimate & correlates. [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/increased-incidence-of-sudden-cardiac-death-in-systemic-sclerosis-estimate-correlates/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/increased-incidence-of-sudden-cardiac-death-in-systemic-sclerosis-estimate-correlates/