Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Despite the high disease burden and reduced quality of life for patients with CTD-ILD, data on its incidence and prevalence – particularly by CTD subtype (RA, SSc, SLE, IIM, MCTD and pSS) – remains limited. This study describes the incidence and prevalence of CTD-ILD and its subtypes in the US.
Methods: This retrospective cohort study (GSK Studies 223907, 224023) of two large US databases (Optum® de-identified Electronic Health Record data set [Optum® EHR], and MarketScan® Commercial and Medicare Databases [MarketScan]) identified adults with CTD-ILD subgroups of interest between January 2018 and December 2023, using ICD-10 diagnosis codes and algorithms, in a two-step process: 1) identifying individuals with CTD, and 2) identifying ILD on or within 365 days before or after the CTD diagnosis. Index date: the later date of the first CTD or ILD diagnosis. Identified CTD-ILD cases were classified as prevalent. Of those, incident cases required a 1-year enrolment prior to index with no ILD claims during this “washout” period. Incidence was presented per 100,000 person-years (PY) and prevalence per 100,000 persons (comprising crude rates, including stratification by age and sex, and age- and sex-adjusted rates).
Results: Among all patients with CTD-ILD identified (Nf20,276 Optum® EHR and Nf9342 MarketScan), most were female (Optum® EHR: 74.1%; MarketScan: 76.0%), with median (interquartile range) age of 65 (56, 73) years (Optum® EHR) and 56 (49, 63) (MarketScan), and had RA-ILD (Optum® EHR: 57.4%, MarketScan: 53.2%). In Optum® EHR, race of patients was 73.2% Caucasian, 16.8% Black, 2.6% Asian, and 7.4% had missing race. Race of patients was not captured in MarketScan.Age- and sex-adjusted rates for CTD-ILD overall were 9.4 (Optum® EHR) and 10.7 (MarketScan) per 100,000 PY for incidence (Table 1), and 45.1 (Optum® EHR) and 44.5 (MarketScan) per 100,000 persons for prevalence (Table 2). Age- and sex- adjusted incidence varied by CTD subtype in Optum® EHR (0.7 [MCTD-ILD] to 5.6 [RA-ILD]) and MarketScan (0.7 [MCTD-ILD] to 6.6 [RA-ILD]) (Table 1). This variation also existed for adjusted prevalence rates (Table 2). Crude stratified rates were approximately double in females versus males, and ≥3 × higher in ages 65 and older versus 18–64 years, across all CTD-ILD subtypes (Tables 1 and 2). Incidence and prevalence rates increased over the study period.
Conclusion: The scarcity of US data on CTD-ILD epidemiology underscores the importance of investigating ILD in patients with CTD, and vice versa, to aid diagnosis and intervention, particularly in older patients and females, where CTD-ILD incidence and prevalence rates are highest. Overall, CTD-ILD incidence and prevalence rates were highest for RA-ILD, corresponding to the higher rates of RA compared with other CTD subtypes. Importantly, findings for age- and sex-adjusted rates were similar between these two large US databases capturing different US patient populations. These prevalence data suggest that 116,000–118,000 individuals in the US have CTD-ILD (based on 2023 adult population estimated at 262.1 million). These novel data highlight a substantial healthcare burden, especially in older patients and females.Funding: GSK Original presentation: EULAR 2025
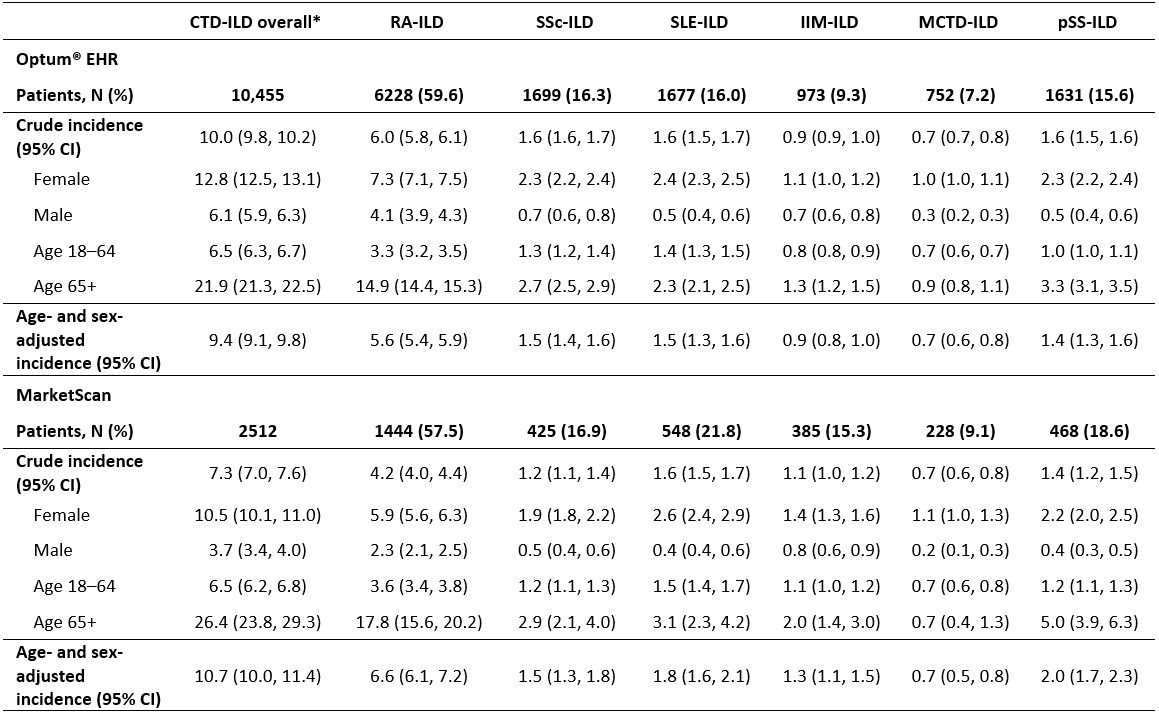 Table 1. Crude and adjusted incidence (per 100,000 person-years) of CTD-ILD – overall and in CTD-ILD subgroups of interest – in US Optum® EHR and MarketScan databases.
Table 1. Crude and adjusted incidence (per 100,000 person-years) of CTD-ILD – overall and in CTD-ILD subgroups of interest – in US Optum® EHR and MarketScan databases.
*Overall captures any CTD-ILD (no duplicates), using ICD-10 diagnosis codes. Patients may be captured in more than 1 CTD subtype but will contribute only once to the CTD-ILD overall column.
CI, confidence interval; CTD, connective tissue diseases; EHR, electronic health record; ICD-10, International Classification of Diseases 10th Revision; IIM, idiopathic inflammatory myositis; ILD, interstitial lung disease; MCTD, mixed connective tissue disease; pSS, primary Sjögren’s syndrome; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSc, systemic sclerosis.
.jpg) Table 2. Crude and adjusted prevalence (per 100,000 persons) of CTD-ILD – overall and in CTD-ILD subgroups of interest – in US Optum® EHR and MarketScan databases.
Table 2. Crude and adjusted prevalence (per 100,000 persons) of CTD-ILD – overall and in CTD-ILD subgroups of interest – in US Optum® EHR and MarketScan databases.
*Overall captures any CTD-ILD (no duplicates), using ICD-10 diagnosis codes. Patients may be captured in more than 1 CTD subtype but will contribute only once to the CTD-ILD overall column.
CI, confidence interval; CTD, connective tissue diseases; EHR, electronic health record; ICD-10, International Classification of Diseases 10th Revision; IIM, idiopathic inflammatory myositis; ILD, interstitial lung disease; MCTD, mixed connective tissue disease; pSS, primary Sjögren’s syndrome; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSc, systemic sclerosis.
To cite this abstract in AMA style:
Martins D, Mu G, Irving E, Levy R, Bhatt N, Wurst K. Incidence and Prevalence of Connective Tissue Diseases with Interstitial Lung Disease (CTD-ILD) in the United States [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/incidence-and-prevalence-of-connective-tissue-diseases-with-interstitial-lung-disease-ctd-ild-in-the-united-states/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/incidence-and-prevalence-of-connective-tissue-diseases-with-interstitial-lung-disease-ctd-ild-in-the-united-states/