Session Information
Date: Monday, November 6, 2017
Title: Rheumatoid Arthritis – Human Etiology and Pathogenesis Poster II
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with RA harbor autoantibodies of various isotypes and directed against several post-translational modifications. Baseline seropositivity is a poor prognostic factor for sustained drug-free remission (SDFR). However, autoantibody levels may change and patients may become seronegative under treatment. It is unknown how often this happens, and whether decreasing levels or becoming seronegative early in disease, indicating disappearance of serological autoimmunity, improves chances of SDFR. To investigate this, we measured a large variety of autoantibodies, including isotypes, in RA patients over time and investigated whether changes in their levels and/or presence associated with SDFR.
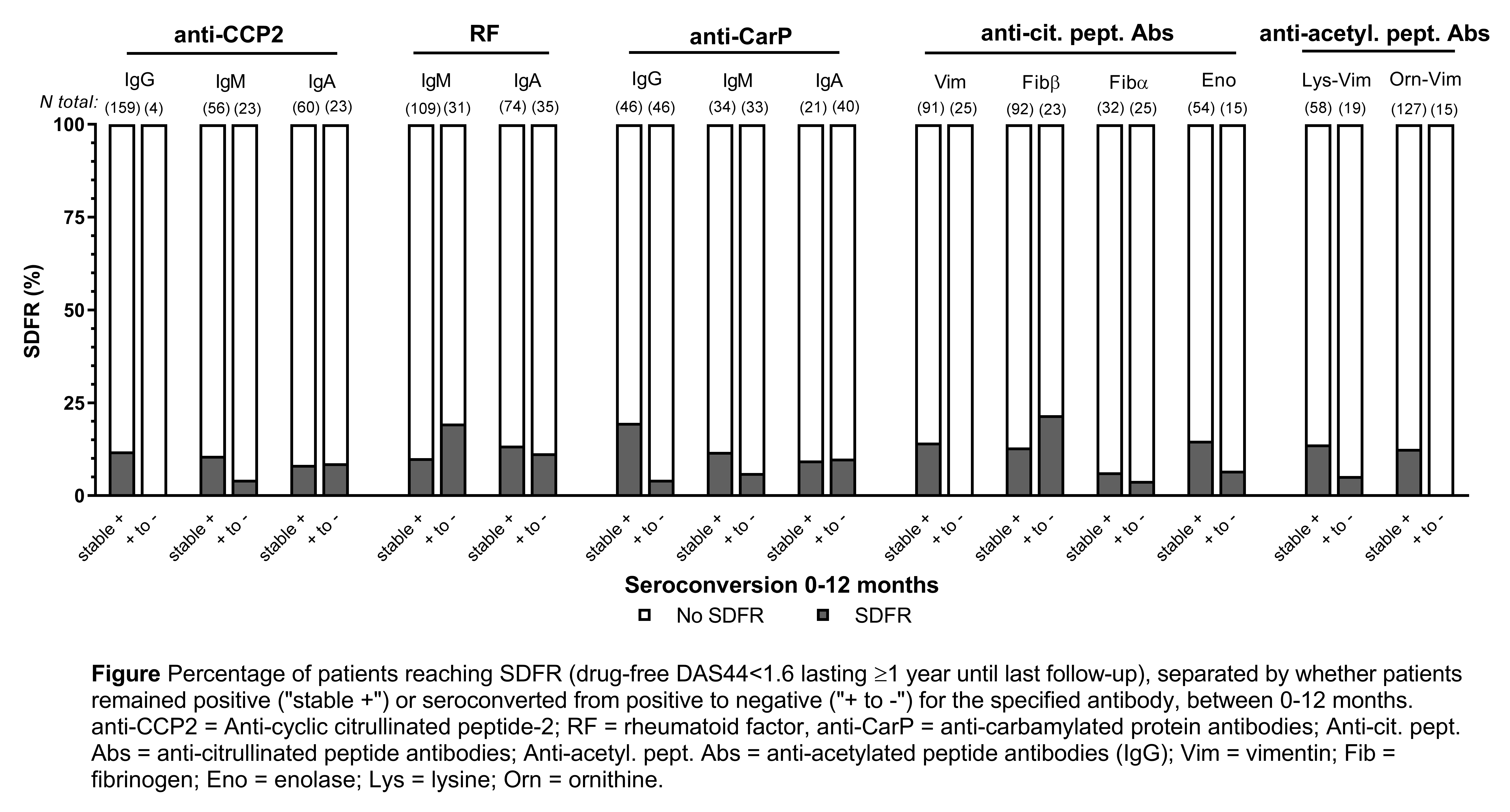
Methods: In sera of 381 seropositive RA patients in the IMPROVED study1, we measured, at 4 month intervals over the first year of treatment: IgG, IgM, and IgA isotypes for anti-cyclic citrullinated peptide-2, rheumatoid factor, anti‐carbamylated protein antibodies, and autoantibodies against 4 citrullinated and 2 acetylated peptides. We investigated whether changes in antibody levels and seroconversion from positive to negative for each individual antibody was favorable for SDFR (drug-free DAS44<1.6 lasting ≥1 year until last follow-up).
Results: For all 14 antibodies, median levels decreased significantly between baseline and 4 months and then stabilized. The prevalence of seroconversion from positive to negative between 0-12 months varied substantially depending on the autoantibody and occurred in 3% (anti-CCP2 IgG) to 66% (anti-CarP IgA) of patients positive at baseline. We hypothesized that greater level decreases and seroconversion, reflecting disappearance of the underlying immunopathology, might be favorable for the long-term outcome SDFR, an outcome approximating disease curation. Surprisingly, greater median decreases in levels were not associated with higher chance of SDFR. Furthermore, we found no evidence that rates of SDFR were higher in patients who seroconverted compared those who stayed seropositive, for all antibodies analyzed (see Figure).
Conclusion: Autoantibody levels decrease and seroconversion from positive to negative occurs under treatment, but these changes do not seem to translate to apparent clinical long-term benefits with regard to SDFR. This suggests that in these patients, despite the disappearance of measurable serological autoimmunity, other immunopathological processes sustain the disease.
References:
1Heimans, AR&T 2016, 18:23.
To cite this abstract in AMA style:
de Moel E, Derksen V, Trouw L, Bang H, Goekoop-Ruiterman YP, Steup-Beekman G, Huizinga TWJ, Allaart CF, Toes REM, van der Woude D. In RA, Becoming Seronegative over the 1st Year of DMARD Treatment Does Not Improve Chances of Drug-Free Remission in the Long-Term [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/in-ra-becoming-seronegative-over-the-1st-year-of-dmard-treatment-does-not-improve-chances-of-drug-free-remission-in-the-long-term/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/in-ra-becoming-seronegative-over-the-1st-year-of-dmard-treatment-does-not-improve-chances-of-drug-free-remission-in-the-long-term/