Session Information
Date: Monday, November 9, 2020
Title: SLE – Diagnosis, Manifestations, & Outcomes Poster III: Bench to Bedside
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Tryptophan (TRP) is metabolized to kynurenine (KYN), quinolonic acid [QA, a N-methyl D-aspartate receptor (NMDAR) agonist] and kynurenic acid (KA, an NMDAR antagonist). KYN/TRP pathway stimulation by IFNa may create a potential neurotoxic QA/KA imbalance in SLE. We investigated QA/KA ratios in SLE subjects vs. healthy controls (HC) and their associations with cognition and depression.
Methods: We recruited 74 SLE subjects who met ACR criteria and had no focal neurologic or primary neuropsychiatric (NP) disorders and 74 HC. We assessed cognition and mood with the Automated Neuropsychological Assessment Metrics (ANAM), depression with the Beck Depression Index, and serum levels of KYN, TRP, QA, and KA with HPLC. Exclusion criteria included alcohol or illicit drug abuse, infection, and current narcotic/psychiatric medication use. SLE disease activity (DA) was defined as Inactive [clinical SLEDAI=0 and PGA≤0.5 and prednisone≤10 mg, and lack of flare on the SELENA-SLEDAI Flare Index]; Stable Active (clinical SLEDAI >0 or PGA >0.5 or prednisone >10 mg and lack of flare) or Flare (mild/moderate or severe flare on the Flare Index). We assessed differences in demographic and clinical characteristics, NP test scores, and KYN/TRP pathway metabolites between SLE and HC and among the SLE DA groups, and the association of variables with NP performance (Spearman’s correlation/t-test/Mann-Whitney/ANOVA/Kruskal-Wallis/chi square/Fisher’s exact test). Multivariable modeling was used to assess the impact of variables on NP task performance in SLE and HC combined, and SLE only; variables on univariate screen (p< 0.1) were included.
Results: There were no demographic or educational differences in SLE vs. HC. SLE subjects performed worse than HC on all behavioral tasks and most cognitive tests (Table 1). Among SLE, there was a significant positive correlation between SLEDAI and MTS scores (r = 0.236, p=0.04), SLE with active disease had higher depression scores vs. Inactive (p< 0.01) and Inactive trended towards worse scores on most cognitive tests vs. Flare. Prednisone dose did not associate with cognitive or depression scores. Serum KYN/TRP and QA/KA ratios were elevated in SLE vs. HC (p< 0.01) (Fig. 1A), and there were no differences in either ratio among SLE DA groups (Fig. 1B). In SLE and HC combined, elevated QA/KA significantly correlated with increased SRT (r = 0.217, p< 0.01), poor performance on MTS (r = -0.307, p< 0.01) and RMCPT (r = -0.311, p< 0.01), and with higher depression scores (r = 0.335, p< 0.01) (Table 1). In SLE alone, an elevated QA/KA correlated with poor performance on MTS (r = -0.237, p=0.04), and trended towards slightly higher odds of depression (OR = 1.03, 95% CI=0.99-1.06, p=0.09). Multivariable modeling revealed that the QA/KA ratio negatively impacted MTS scores (Table 2), while increased SLEDAI had a positive impact.
Conclusion: Elevated serum KYN/TRP and QA/KA ratios indicate KYN/TRP pathway activation in SLE. Surprisingly, DA associated with improved cognitive performance. An increased QA/KA ratio, after controlling for other factors, associated with poor cognitive performance on a working memory task, supporting its further study as a potential biomarker for SLE-related cognitive dysfunction.
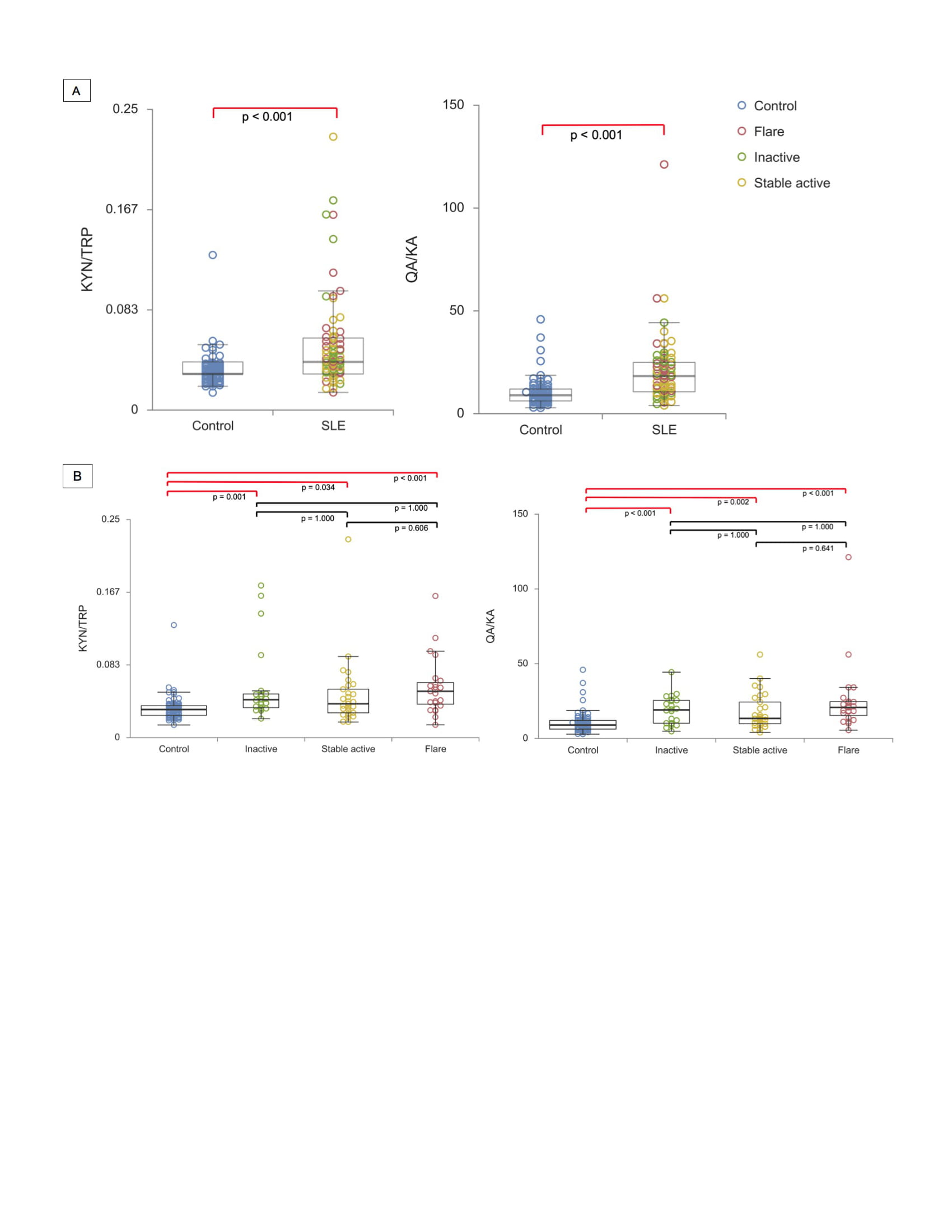 Figure 1: Serum KYN/TRP pathway metabolite ratios in SLE subjects and healthy controls (HC). The serum KYN/TRP and QA/KA ratios measured by HPLC are displayed both in all SLE subjects compared to HC (A) and in SLE subjects grouped by disease activity and HC (B). Circles represent a particular subject, and the color represents the disease activity group of that subject.
Figure 1: Serum KYN/TRP pathway metabolite ratios in SLE subjects and healthy controls (HC). The serum KYN/TRP and QA/KA ratios measured by HPLC are displayed both in all SLE subjects compared to HC (A) and in SLE subjects grouped by disease activity and HC (B). Circles represent a particular subject, and the color represents the disease activity group of that subject.
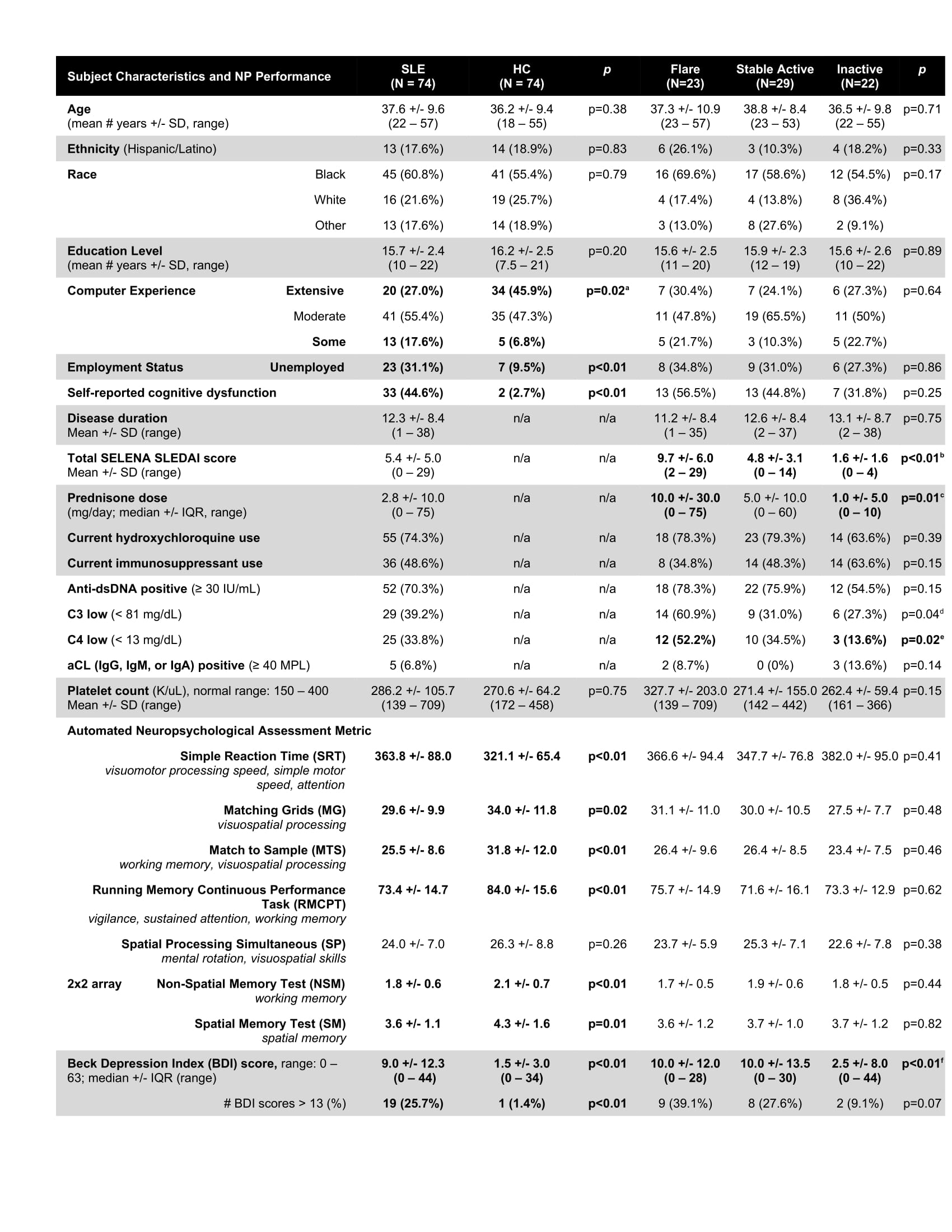 Table 1: SLE subject and healthy control (HC) characteristics and neuropsychological (NP) test performance. All data is reported either as a mean (or median where indicated) +/- standard deviation (or interquartile range), or as a frequency (%). All data refers to that which was collected at the time of evaluation. Data comparing SLE and HC, as well as comparisons among SLE disease activity groups, are displayed. a. Extensive and Some (p=0.009) b. Flare and Inactive (p=0.000), Flare and Stable Active (p=0.000), Stable Active and Inactive (p=0.019) c. Flare and Inactive (p=0.004) d. No significant differences among groups after correction for multiple comparisons e. Flare and Inactive (p=0.006) f. Flare and Inactive (p=0.002), Stable Active and Inactive (p=0.029)
Table 1: SLE subject and healthy control (HC) characteristics and neuropsychological (NP) test performance. All data is reported either as a mean (or median where indicated) +/- standard deviation (or interquartile range), or as a frequency (%). All data refers to that which was collected at the time of evaluation. Data comparing SLE and HC, as well as comparisons among SLE disease activity groups, are displayed. a. Extensive and Some (p=0.009) b. Flare and Inactive (p=0.000), Flare and Stable Active (p=0.000), Stable Active and Inactive (p=0.019) c. Flare and Inactive (p=0.004) d. No significant differences among groups after correction for multiple comparisons e. Flare and Inactive (p=0.006) f. Flare and Inactive (p=0.002), Stable Active and Inactive (p=0.029)
 Table 2: Results of multivariable analysis to determine predictors of neuropsychological test performance. Results of multivariable models that included all subjects (“SLE and HC combined,” top section) and those that included only SLE subjects (“SLE Only,” bottom section) are displayed. Variables with a significant, negative impact on a particular ANAM test (see Table 1) are indicated with an “X.” The Spatial Processing (SP) test column is grayed-out since SLE subjects did not perform significantly worse than HC on this test. # All of the test scores were significantly lower in SLE compared to HC except for the Spatial Processing test (SP) *p < 0.05 **p < 0.01
Table 2: Results of multivariable analysis to determine predictors of neuropsychological test performance. Results of multivariable models that included all subjects (“SLE and HC combined,” top section) and those that included only SLE subjects (“SLE Only,” bottom section) are displayed. Variables with a significant, negative impact on a particular ANAM test (see Table 1) are indicated with an “X.” The Spatial Processing (SP) test column is grayed-out since SLE subjects did not perform significantly worse than HC on this test. # All of the test scores were significantly lower in SLE compared to HC except for the Spatial Processing test (SP) *p < 0.05 **p < 0.01
To cite this abstract in AMA style:
Anderson E, Fishbein J, Hong J, Roeser J, Furie R, Aranow C, Volpe B, Diamond B, Mackay M. Impact of the Kynurenine/Tryptophan Pathway on Cognitive Dysfunction and Depression in Systemic Lupus Erythematosus [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/impact-of-the-kynurenine-tryptophan-pathway-on-cognitive-dysfunction-and-depression-in-systemic-lupus-erythematosus/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/impact-of-the-kynurenine-tryptophan-pathway-on-cognitive-dysfunction-and-depression-in-systemic-lupus-erythematosus/