Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Infections have been implicated as potential triggers for autoimmune responses, but studies primarily focused on the history of infection linked with autoimmune diseases. Large-scale longitudinal studies on antibodies to infections and their associations with autoimmune diseases are limited. By exploring associations between seropositivity to infection and prevalent and incident autoimmune diseases, we aim to better understand the etiologic role of infection in autoimmune diseases.
Methods: We analyzed data on serum samples from 9,429 randomly selected UK Biobank participants who have been tested for 45 antibody responses to 20 pathogens (human herpes [HHV], hepatitis, polyoma, papilloma [HPV] and retroviruses, as well as Chlamydia trachomatis, Helicobacter pylori, Toxoplasma gondii) using a bead-based multiplex platform. The association between seropositivity and autoimmune diseases was assessed with multivariable odds ratios (ORs) and 95% confidence intervals (CIs) using logistic regression for prevalent and multivariable hazard ratios (HRs) and 95% CIs using Cox regression for incident cases. Forty-eight autoimmune diseases were ascertained using ICD codes and self-reported diagnosis. Multiple testing was adjusted using Bonferroni correction.
Results: 517 (5.5%) had at least one autoimmune disease at baseline (59% women). Among individuals with autoimmune diseases, BKV showed the highest seropositivity (96.5%) and HIV-1 the lowest (0%). Seropositivity to JCV was associated with any prevalent autoimmune disease in both sexes (OR [95% CI] 1.40 [1.08-1.80]); antibodies to hepatitis B virus (HBV) with Graves’ disease (GD) in men (17.99 [3.93-82.00]) and HHV-7 with polymyalgia rheumatica (PR) in women (0.14 [0.04-0.43]). Among nominal significance (p< 0.05), OR ranged from 0.22 (HHV-7/ PR) to 6.42 (HBV/GD) in both sexes; 0.13 (HHV-6/ankylosing spondylitis [AS]) to 10.18 (HTLV-1/AS) in men; 0.18 (HHV-7/rheumatism) to 29.96 (HBV/AS) in women. Of 8,912 autoimmune disease-free individuals, 679 developed new autoimmune diseases (median follow-up 7.5 years). Baseline seropositivity to herpes simplex virus-1 (HSV-1) was inversely associated with aplastic anemia (AA) (HR 0.10 [95% CI 0.02-0.32]). HRs for nominal association ranged from 0.18 (BKV/sarcoidosis) to 12.37 (HCV/ulcerative colitis (UC)) in both sexes; 0.07 (HSV-1/pernicious anemia) to 23.07 (HCV/UC) in men, 0.08 (HHV-7/vasculitis) to 149.07 (HIV-1/primary sclerosing cholangitis) in women.
Conclusion: Our study provides a comprehensive investigation of antibodies to infectious agents and autoimmune diseases in a population cohort. Inverse associations indicate that infections may modulate the immune system and suppress pro-inflammatory processes or could reflect an altered immune status of the host. Conversely, positive associations suggest that infections could trigger autoimmunity through mechanisms like molecular mimicry. By elucidating these pathogen associations, our research significantly advances our understanding of autoimmune disease etiology and provides insights for targeted interventions to reduce infection-related autoimmune risks.
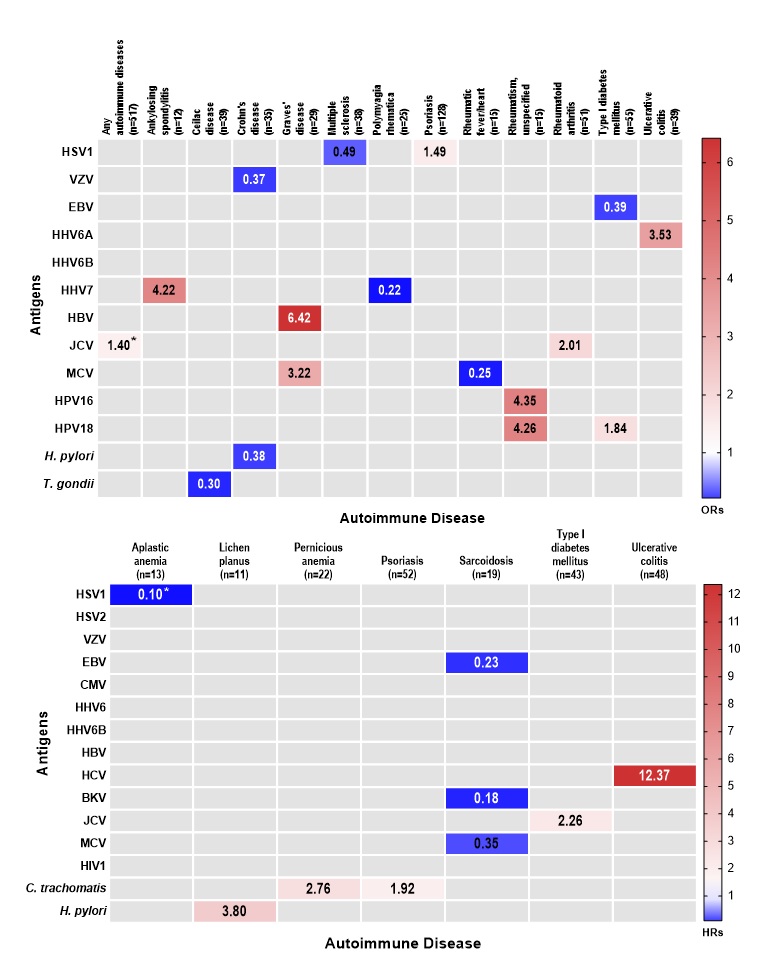
The numbers represent odds ratios (top)/hazard ratios (bottom)
*Significant at Bonferroni cut-off (p<0.002272727)
HSV1: Herpes Simplex virus_1, HSV2: Herpes Simplex virus_2, VZV: Varicella Zoster Virus, EBV: Epstein-Barr Virus, CMV: Human Cytomegalovirus, HHV6: Human Herpesvirus-6, HHV6A: Human Herpesvirus-6A, HHV6B: Human Herpesvirus-6B, HHV7: Human Herpesvirus-7, HBV: Hepatitis B Virus, HCV: Hepatitis C Virus, BKV: Human Polyomavirus BKV, JCV: Human Polyomavirus JCV, MCV: Merkel Cell Polyomavirus MCV, HPV16: Human Papillomavirus type_16, HPV18: Human Papillomavirus type_18, HIV1: Human Immunodeficiency Virus, C. trachomatis: Chlamydia trachomatis, H. pylori: Helicobacter pylori, T. gondii: Toxoplasma gondii
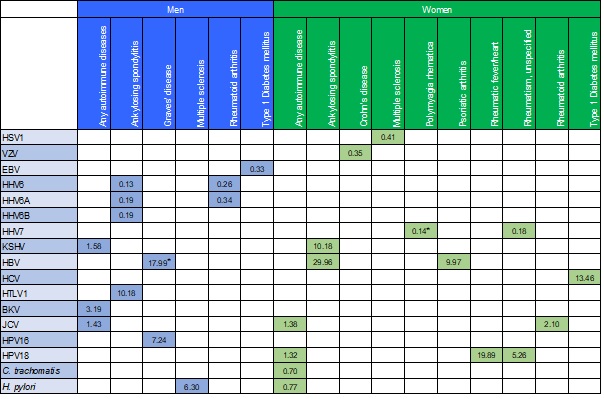
The numbers represent odds ratios
*Significant at Bonferroni cut-off (p<0.002272727)
HSV1: Herpes Simplex virus_1, VZV: Varicella Zoster Virus, EBV: Epstein-Barr Virus, HHV6: Human Herpesvirus-6, HHV6A: Human Herpesvirus-6A, HHV6B: Human Herpesvirus-6B, HHV7: Human Herpesvirus-7, KSHV: Kaposi’s Sarcoma-Associated Herpesvirus, HBV: Hepatitis B Virus, HCV: Hepatitis C Virus, BKV: Human Polyomavirus, HTLV1: Human T-Lymphotropic Virus_1, BKV: Human Polyomavirus BKV, JCV: Human Polyomavirus JCV, HPV16: Human Papillomavirus type_16, HPV18: Human Papillomavirus type_18, HIV1: Human Immunodeficiency Virus, C. trachomatis: Chlamydia trachomatis, H. pylori: Helicobacter pylori
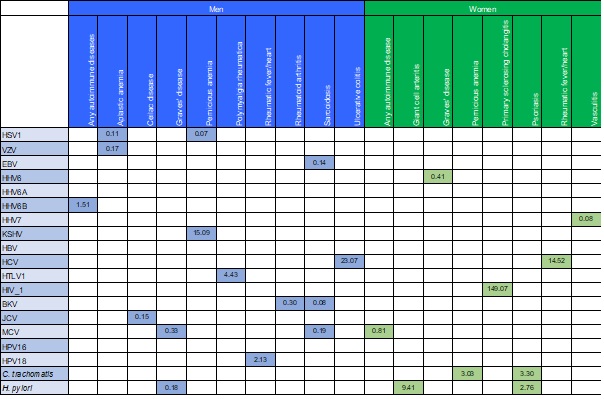
The numbers represent hazard ratios
HSV1: Herpes Simplex virus_1, VZV: Varicella Zoster Virus, EBV: Epstein-Barr Virus, HHV6: Human Herpesvirus-6, HHV6A: Human Herpesvirus-6A, HHV6B: Human Herpesvirus-6B, HHV7: Human Herpesvirus-7, KSHV: Kaposi’s Sarcoma-Associated Herpesvirus, HBV: Hepatitis B Virus, HCV: Hepatitis C Virus, HTLV1: Human T-Lymphotropic Virus_1, HIV1: Human Immunodeficiency Virus, BKV: Human Polyomavirus, JCV: Human Polyomavirus JCV, MCV: Merkel Cell Polyomavirus MCV, HPV16: Human Papillomavirus type_16, HPV18: Human Papillomavirus type_18, C. trachomatis: Chlamydia trachomatis, H. pylori: Helicobacter pylori
To cite this abstract in AMA style:
Yun C, Beydoun M, Launer L, Song M. Immune Responses to Infection and Autoimmune Diseases in the UK Biobank [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/immune-responses-to-infection-and-autoimmune-diseases-in-the-uk-biobank/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/immune-responses-to-infection-and-autoimmune-diseases-in-the-uk-biobank/