Session Information
Date: Monday, November 18, 2024
Title: Osteoporosis & Metabolic Bone Disease – Basic & Clinical Science Poster
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Axial spondyloarthritis (AxSpA) is characterized by abnormal bone formation and, paradoxically, bone loss accompanied by increased bone fragility and vertebral fracture risk. Tumor necrosis factor inhibitor (TNFi) and interleukin-17 (IL-17) blockade improve AxSpA symptoms. TNFi therapy is associated with improved BMD but with less clear effects on fracture reduction.1 Our study aimed to determine whether initiation of IL-17 blockade affects bone turnover and bone mineral density (BMD) in patients with AxSpA, and evaluate rates of incident vertebral fractures.
Methods: Patients with radiographic AxSpA beginning therapy with secukinumab were prospectively enrolled. Clinical factors and biomarkers of bone turnover and disease activity (alkaline phosphatase, osteocalcin, IL-17) were assessed at baseline, 2-, 12-, and 24-months. Skeletal assessments collected at baseline, 12-, and 24-months included lateral radiographs, areal BMD (aBMD) and trabecular bone score (TBS) measured via dual energy x-ray absorptiometry (DXA), and volumetric BMD (vBMD) microarchitecture measured by high resolution peripheral quantitative computed tomography (HR-pQCT, Xtreme CT2). Changes in these parameters were assessed by Wilcoxon and paired t-tests. The presence of vertebral fractures was assessed through examination of lateral spine images measured over course of study, and DXA, magnetic resonance imaging, and computed tomography scans were used when vertebrae were not visualized on x-ray.
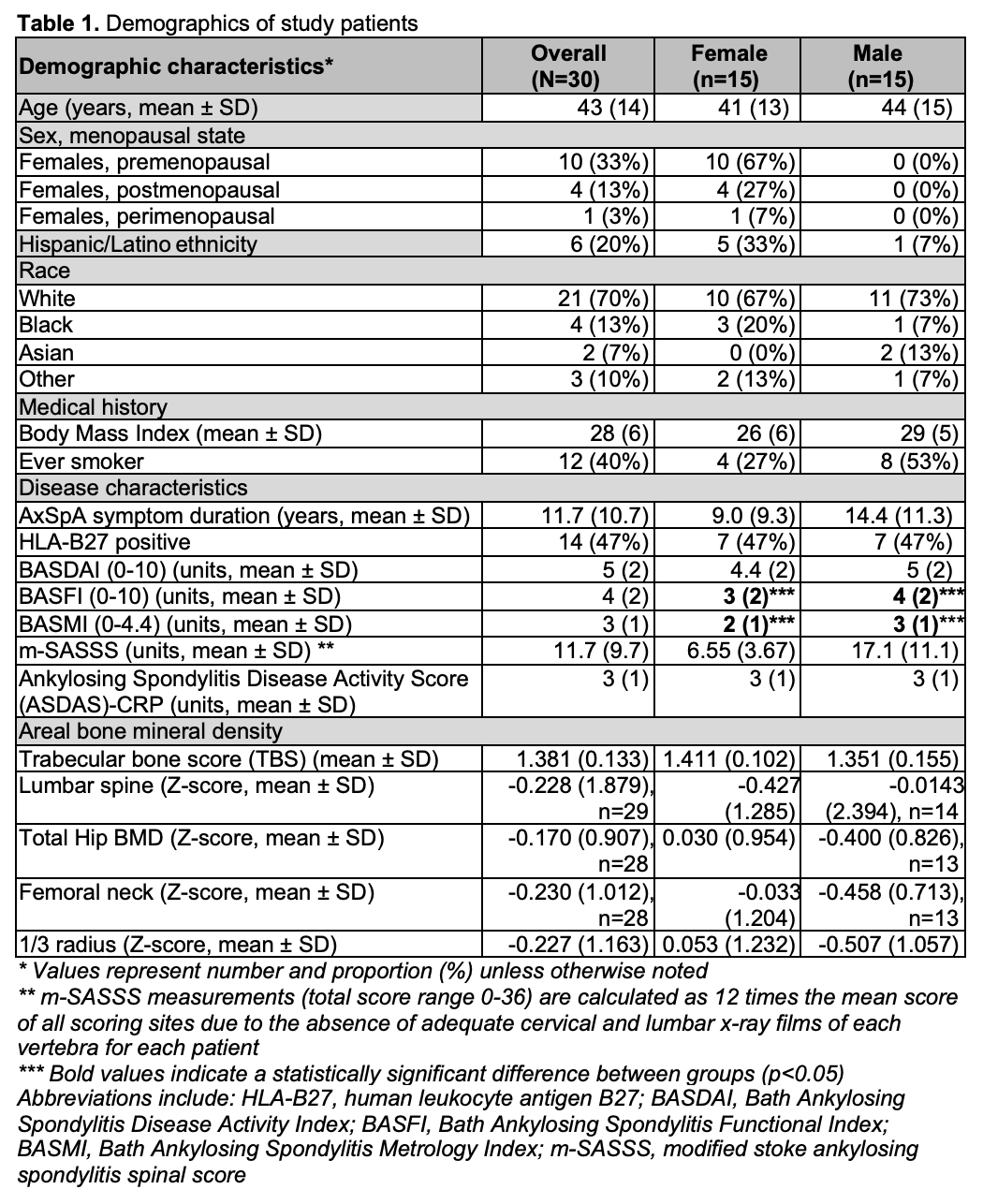
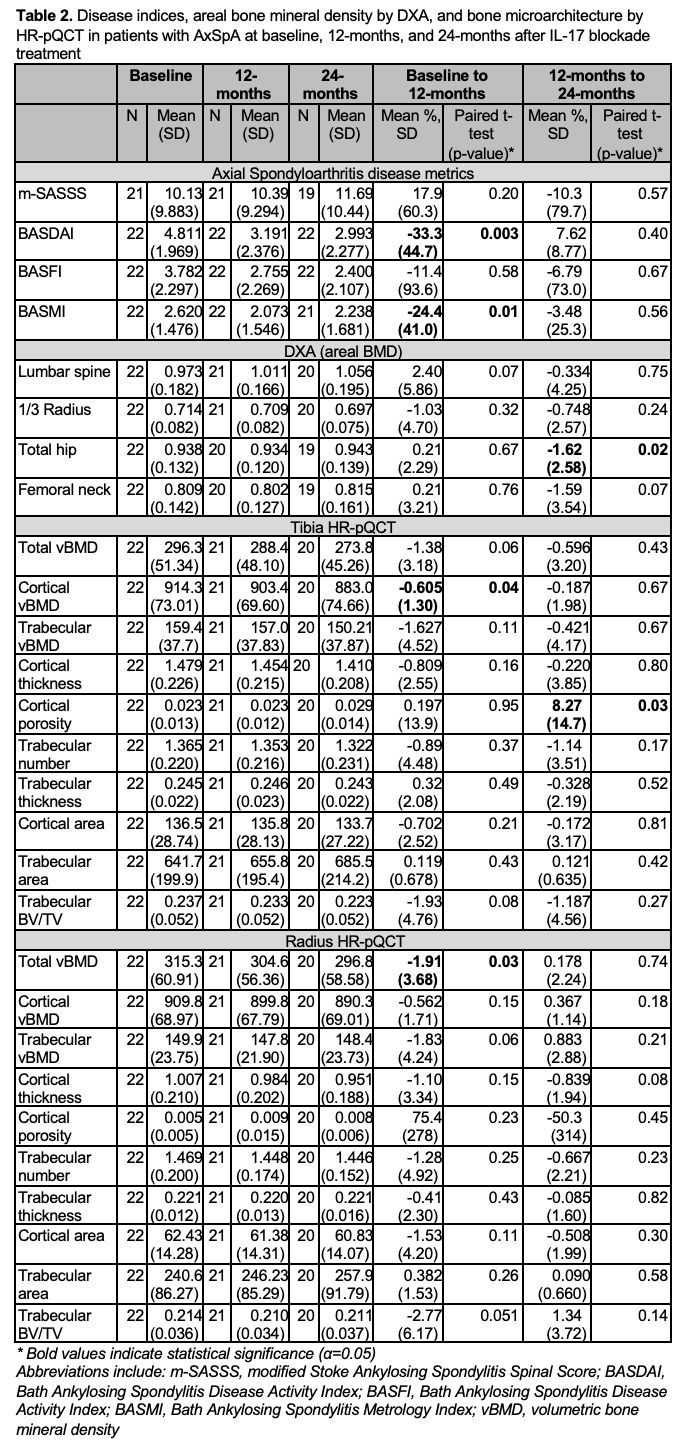
Results: In our cohort of 30 AxSpA subjects, 50% were female (67% premenopausal) and 70% were White. Mean AxSpA symptom duration was 12 years and 47% were HLA-B27 positive (Table 1). Baseline disease activity was moderate (mean Bath Ankylosing Spondylitis Disease Activity Score 5 [SD=2]). Treatment with IL-17 blockade therapy improved activity and function over the first 12-months, with a decrease in BASDAI and Bath Ankylosing Spondylitis Metrology Index Scores (-33.3%, p=0.003 and -24.4%, p=0.01, respectively), then remained stable between 12- and 24-months (Table 2). There were few changes in skeletal indices. Hip aBMD remained stable for the first 12-months before decreasing from 12- to 24-months (-1.6%, p=0.02), but no other change was observed by DXA. HR-pQCT demonstrated small declines in cortical bone at the tibia. Cortical vBMD decreased over the first 12-months (-0.61%, p=0.04), and was stable from 12- to 24-months. Cortical porosity was stable over the first 12-months, then increased between 12- and 24-months (8.3%, p=0.03). At the radius, total vBMD decreased over the first 12-months (-1.9%, p=0.03), then remained stable.
There were no relevant changes in the biomarker panel over 24-months of therapy.
No new vertebral fractures were identified in subjects in spine images captured across 24-months of IL-17 blockade therapy.
Conclusion: In our study, patients with moderate disease activity beginning IL-17 blockade therapy had improvements in clinical symptoms with minimal changes in bone turnover, BMD or microarchitecture.and no increase in vertebral fractures. Future, longer-term controlled studies are needed to further assess the impact of this therapy on skeletal health.
1. Beek JK, et al. PMID 30690799.
To cite this abstract in AMA style:
Heiting C, McMahon D, Mintz D, Yuan W, Mannstadt I, A Russell L, Stein E, Ashany D, Goodman S. IL-17 Blockade Therapy Improves Symptoms in Patients with Active Axial Spondyloarthritis Without Occurrence of New Vertebral Fractures [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/il-17-blockade-therapy-improves-symptoms-in-patients-with-active-axial-spondyloarthritis-without-occurrence-of-new-vertebral-fractures/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/il-17-blockade-therapy-improves-symptoms-in-patients-with-active-axial-spondyloarthritis-without-occurrence-of-new-vertebral-fractures/