Session Information
Date: Wednesday, November 8, 2017
Title: Osteoarthritis – Clinical Aspects II: Structural Progression and Incidence
Session Type: ACR Concurrent Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: Knee OA is a heterogeneous disease, with some patients experiencing rapid deterioration and others experiencing slow disease progression. Identifying patients likely to experience rapid disease worsening is a top research priority; this would allow better recruitment strategies for clinical trials, optimizing the execution of trials focused on disease modifying drugs, and would help physicians make better treatment decisions.
Methods: We used data from the Osteoarthritis Initiative (OAI), a multicenter, longitudinal, observational study of knee OA. We selected patients with baseline (BL) Kellgren-Lawrence (KL) grade 1 – 3, with knee pain, and with joint space width (JSW) assessed at BL and ≥1 follow-up. Medial minimum JSW was assessed with a fixed-flexion knee radiograph annually through year 4; total follow-up was 9 years. We used latent class growth analysis (LCGA) to identify distinct subgroups of JSW progression. LCGA allows for the modeling of distinct subgroups based on longitudinal trajectory. We included random effects for intercept and slope to allow for within-subject variability. After identifying the number of trajectories, we used logistic regression to assess the association between BL characteristics and JSW trajectory group.
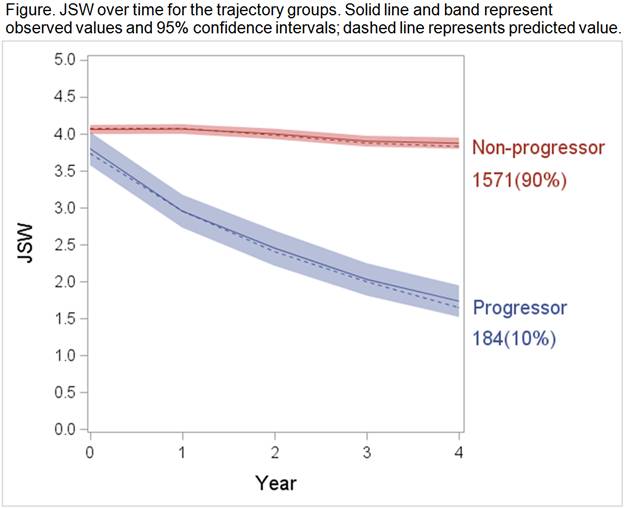
Results: We used data from 1,755 OAI study participants. BL radiographic severity was KL1 in 16%, KL2 in 52%, and KL3 in 32%. The mean (SD) JSW was 4.0mm (1.3) and the range was 0.7 – 8.5mm. LCGA identified 2 distinct JSW trajectories [Figure]. The majority of patients (90%) had stable JSW over 4 years of follow-up (Non-progressor group) with a mean (SD) JSW of 4.1 (1.2) at BL and 3.9 (1.4) at 4 year follow-up, for a yearly decrease of 0.05mm. A subgroup of patients experienced rapid disease progression (Progressor group), with a BL mean (SD) JSW of 3.8 (1.5) and a 4 year follow-up JSW of 1.7 (1.3), for a yearly decrease of 0.53mm. 5% of the Non-progressors went on to have total knee replacement between years 5 and 9, compared to 23% of the Progressors. BL KL, obesity, and alignment were associated with progression group: in a multivariable model, the odds of being a Progressor were 2.4 (95% CI: 1.4, 3.9) times higher for participants with KL 3 vs. KL 1; 1.6 (1.1, 2.1) times higher for obese participants vs. non-obese, and 1.2 (0.8, 1.8) times higher for those with varus alignment vs. neutral. 30% of the cohort had 0 risk factors, 6% were Progressors; 43% had 1 risk factor, 10% were Progressors; 23% had 2 risk factors, 15% were Progressors; 5% had 3 risk factors, 26% were Progressors.
Conclusion: We found a subgroup of patients experiencing rapid structural progression in JSW. These patents may be appropriate candidates for clinical trials of disease modifying drugs. A strategy that required 2 or 3 risk factors for inclusion into a trial could enrich the cohort for progressors by two-fold compared to a strategy of enrolling non-selectively.
To cite this abstract in AMA style:
Collins JE, Katz JN, Losina E. Identifying Rapid Structural Disease Progression in Knee Osteoarthritis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/identifying-rapid-structural-disease-progression-in-knee-osteoarthritis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/identifying-rapid-structural-disease-progression-in-knee-osteoarthritis/