Session Information
Date: Monday, November 13, 2023
Title: (1264–1307) RA – Diagnosis, Manifestations, and Outcomes Poster II
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Current EULAR recommendations for cardiovascular risk (CVR) assessment in rheumatoid arthritis (RA) patients indicate that the CVR evaluation should be performed according to national guidelines; however, there was no algorithm designed for the Mexican population until 2019, when the World Health Organization (WHO) published the CVR charts for 21 world regions, including Mexico. The aim of this study was to determine the capacity of the WHO and other five algorithms for the detection of carotid plaque in RA patients.
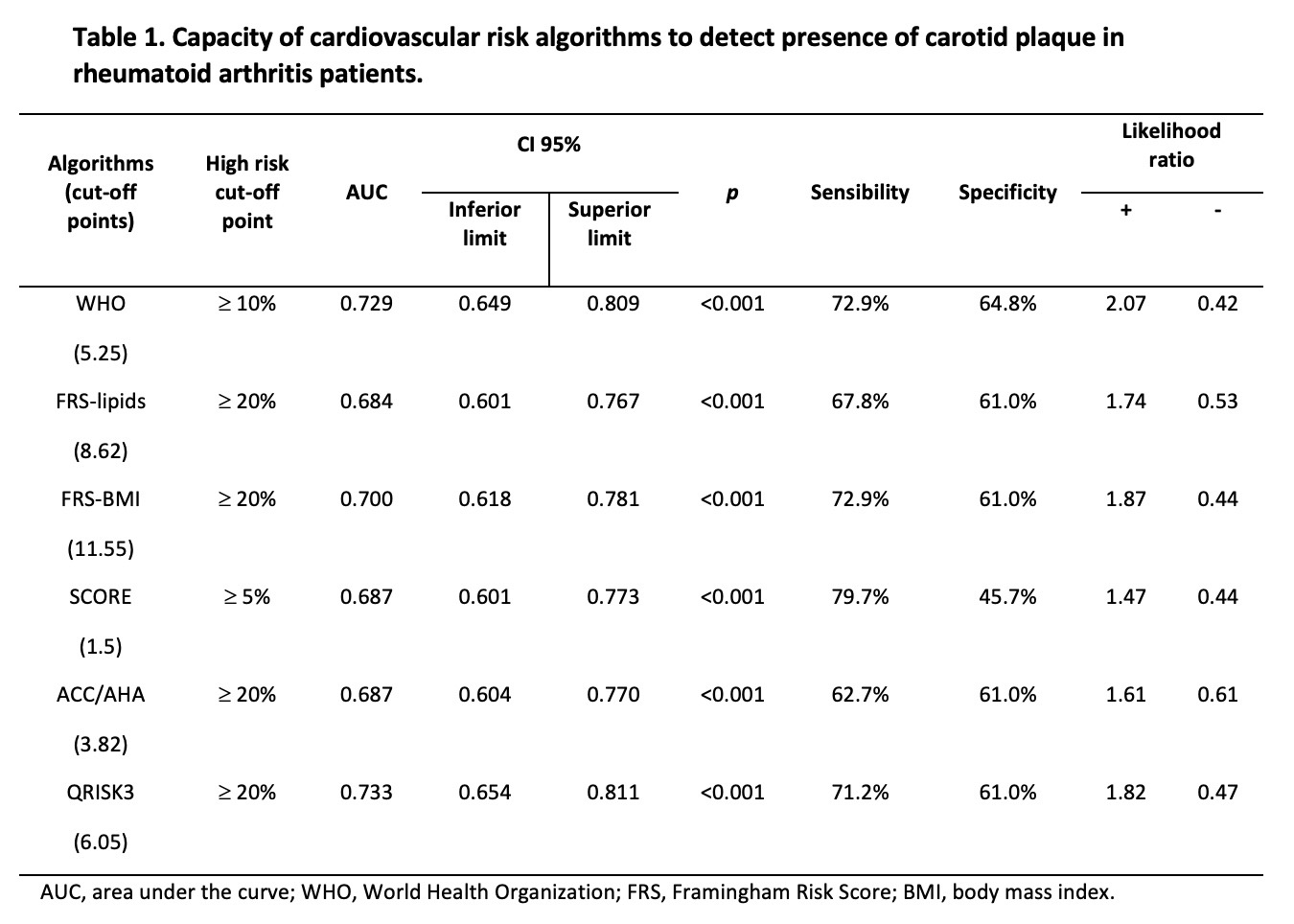
Methods: This was a cross-sectional study. We included 164 patients with RA diagnosis according to the 2010 ACR/EULAR classification criteria, aged 40-75 years. CVR was calculated with six algorithms: WHO, FRS-lipids, FRS-BMI, SCORE, ACC/AHA and QRISK3. The result was multiplied by 1.5, according to current guidelines. Carotid ultrasound was performed to all patients to identify the presence of carotid plaque, which was defined as a cIMT ≥ 1.2 mm or a focal thickness ≥ 0.5 mm. A ROC-curve analysis was performed, and the cutoff points to detect carotid plaque of each algorithm were determined using Youden’s Index. Area under the curve (AUC), sensitivity, specificity, and likelihood ratios were calculated. A p-value < 0.05 was considered statistically significant.
Results: The prevalence of carotid plaque was 35.9%. Mean age was 55.8 ±8.9 years, 156 (95.1%) patients were women, 27 (16.5%) patients had diagnosis of type 2 diabetes mellitus, 53 (32.3%) patients had hypertension, 58 (35.4%) had dyslipidemia, 56 (34.1%) had obesity and 15 (9.1%) were active smokers. The ROC-curve analysis of the algorithms is shown in table 1 and figure 1. All the algorithms tested in this study demonstrated significant discrimination for the presence of carotid plaque, with p-values < 0.001.
Conclusion: Among the various algorithms evaluated, the WHO calculator stood out as one of the most effective tools for detecting carotid plaque, demonstrating superior positive and negative likelihood ratios; however, similar to the other algorithms, a lower cut-off point than the one established by the official guidelines was needed to identify high-risk patients with the presence of CP who were initially classified as low-moderate risk by the CVR algorithm, even though the results were multiplied by 1.5 as established by EULAR recommendations, with the exception of QRISK-3, considering the fact that the disease itself is considered a CVR factor. The utilization of carotid ultrasound remains essential in order to accurately identify high-risk patients and provide them with timely treatment.

To cite this abstract in AMA style:
Guajardo-Jauregui N, Azpiri-López J, Galarza-Delgado D, Colunga I, Cardenas-De la Garza J, Arvizu-Rivera R. Identification of Subclinical Atherosclerosis by Six Cardiovascular Risk Calculators in Rheumatoid Arthritis Patients [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/identification-of-subclinical-atherosclerosis-by-six-cardiovascular-risk-calculators-in-rheumatoid-arthritis-patients/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/identification-of-subclinical-atherosclerosis-by-six-cardiovascular-risk-calculators-in-rheumatoid-arthritis-patients/