Session Information
Date: Saturday, November 16, 2024
Title: SLE – Treatment Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Cardiomyopathy is a rare, life-threatening adverse effect of hydroxychloroquine (HCQ) use. There is a paucity in literature regarding treatment and prognosis in these cases. The aim of this case series is to describe a multi-disciplinary approach to diagnosis, treatment, and outcome of HCQ induced cardiomyopathy.
Methods: IRB approval was obtained. The Montefiore Medical Center electronic medical record database was queried between 2018 – 2023 to identify cardiac pathology cases which showed evidence of HCQ induced cardiomyopathy. Clinical data was obtained from chart review.
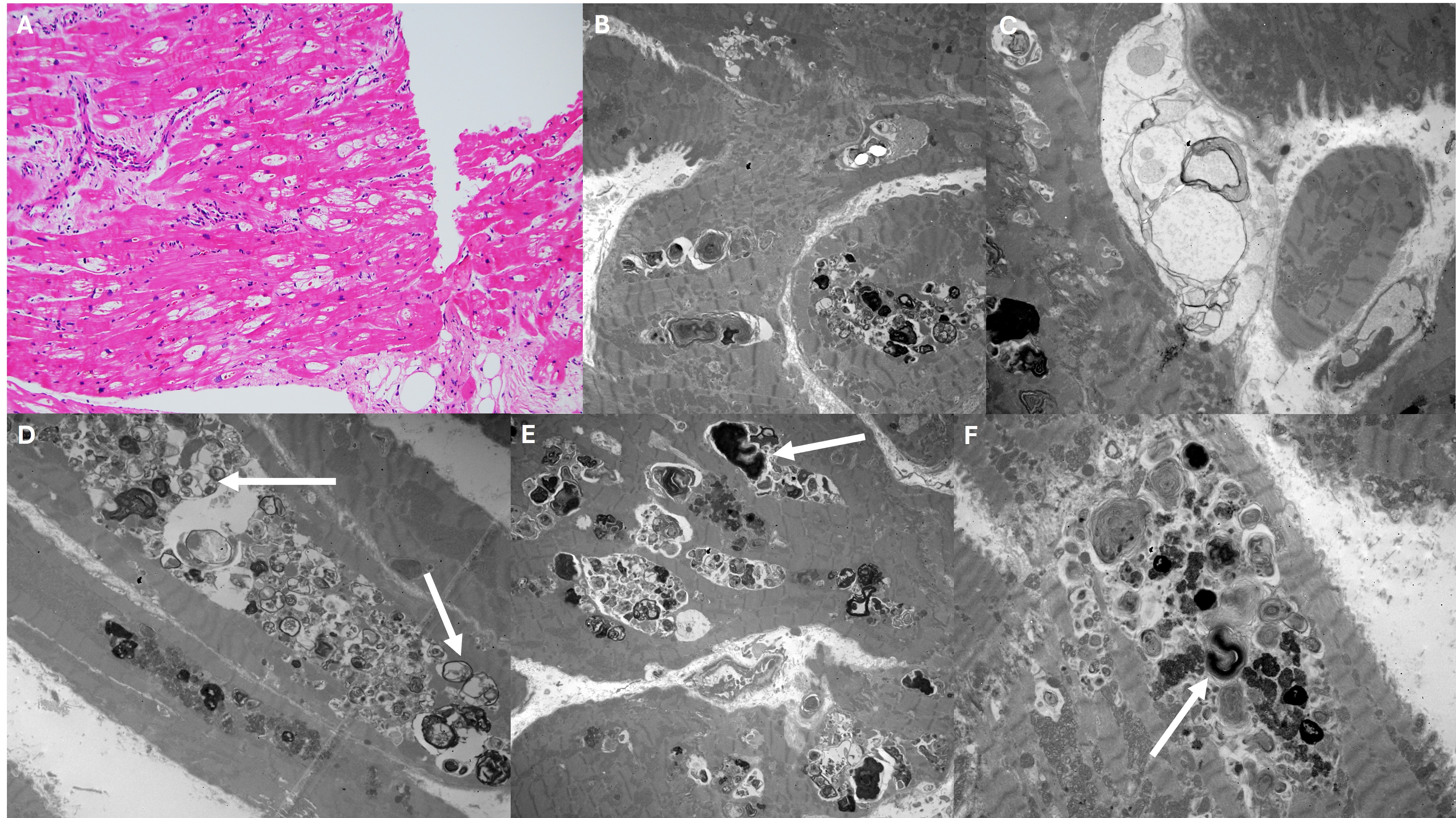
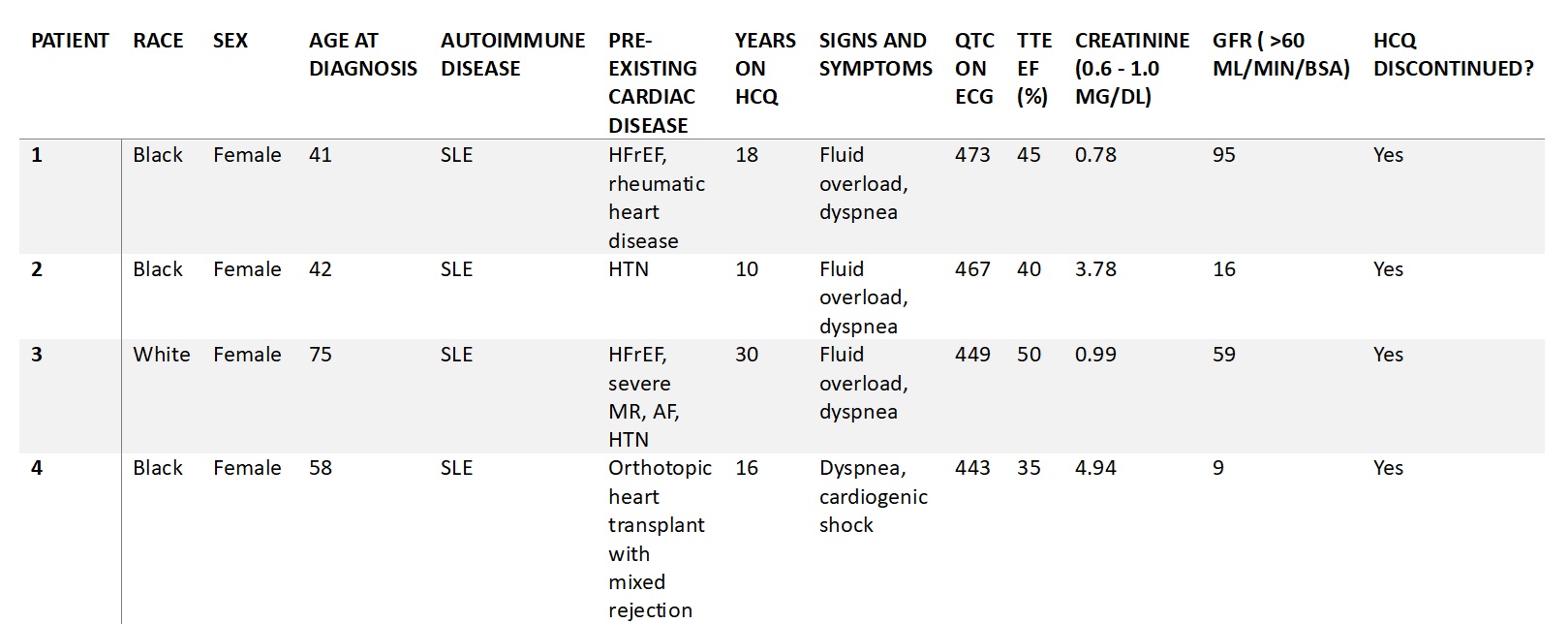
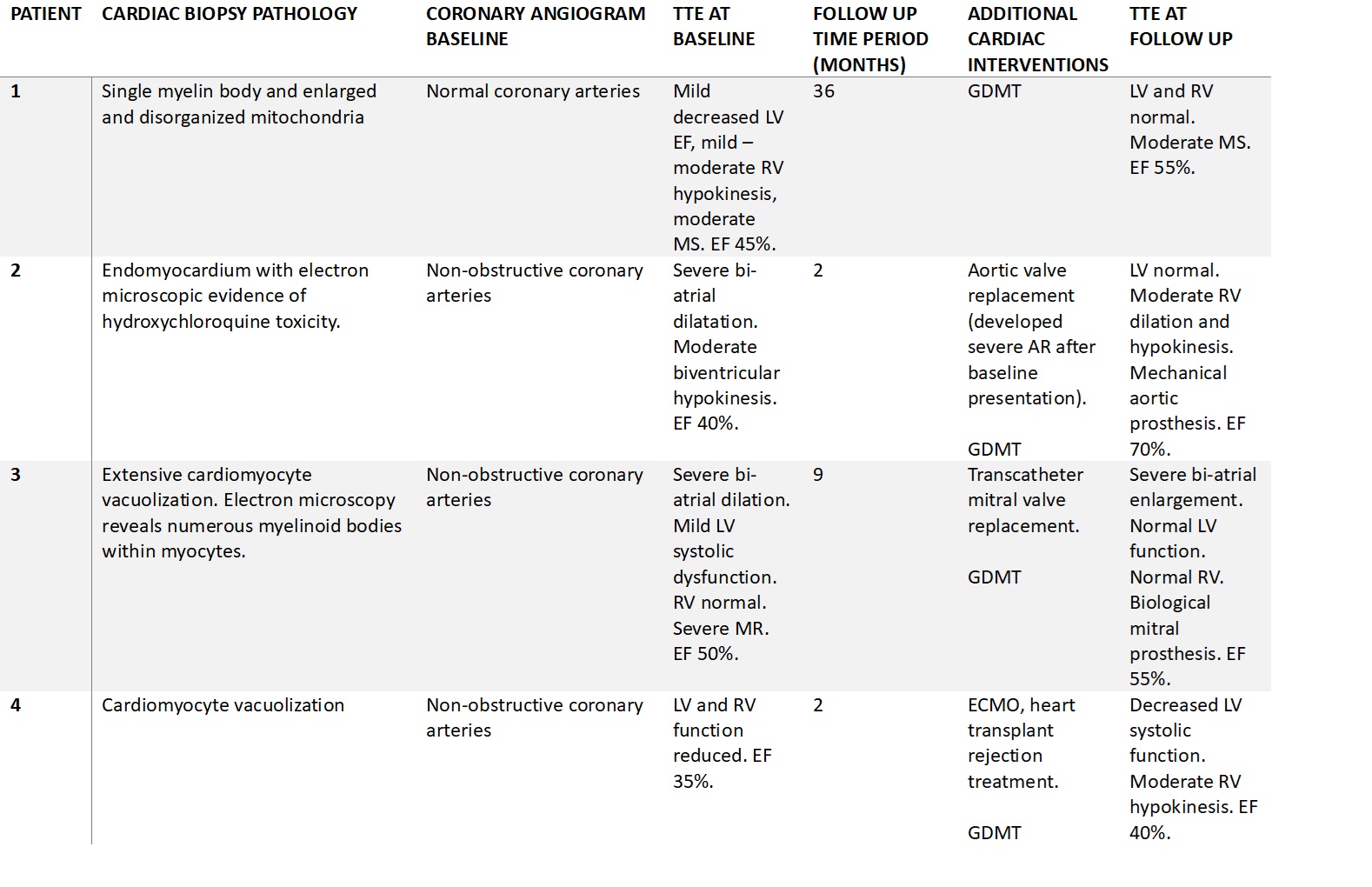
Results: We identified four patients with biopsy proven HCQ cardiotoxicity. Baseline characteristics are summarized in Table 1. The mean age at diagnosis was 54 years. Three patients were African American. All patients were initiated on HCQ for diagnosis of systemic lupus erythematosus, and the average duration of HCQ use was 18.5 years. All patients presented with signs and symptoms of decompensated heart failure with echocardiogram showing reduced ejection fraction. The QTC ranged from 443 to 473. Coronary angiogram was performed in all patients and did not show ischemic cardiomyopathy. Given unclear etiology of heart failure, all patients underwent a cardiac biopsy which showed features of HCQ induced toxicity (Table 2). Figure 1 displays pathology slides from our case series showing cardiomyocyte vacuolization and presence of myelinoid and curvilinear bodies, which are typically seen in HCQ cardiomyopathy. HCQ was permanently discontinued in all cases, and follow up time since cardiac biopsy ranged from 3 to 36 months. The ejection fraction on echocardiogram improved in all patients after discontinuation of HCQ and initiation of guideline directed heart failure treatment, including structural interventions (Table 2).
Conclusion: These cases highlight the high clinical index of suspicion required to diagnose HCQ induced cardiomyopathy. Right ventricle cardiac biopsy showing vacuolization of cardiomyocytes and curvilinear and myelinoid bodies is critical to diagnose this rare entity, since serology and imaging findings were not shown to be specific. Ejection fraction improved for all patients in our case series with permanent discontinuation of HCQ and guideline directed heart failure management. This suggests that HCQ discontinuation alone may not be sufficient in our increasingly complex, multi-morbid patient population, and modern heart failure therapy and cardiac interventions will likely be required to improve cardiac function. A multi-disciplinary approach with heart failure cardiologists, rheumatologists, pathologists, and cardiothoracic surgeons is necessary for the diagnosis and management for these patients. Further studies are needed to help identify risk factors for the development of HCQ cardiomyopathy.
.
To cite this abstract in AMA style:
Tripathy S, Chen D, DiFranza L, Ayesha B. Hydroxychloroquine Induced Cardiomyopathy: A Biopsy Proven Case Series [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/hydroxychloroquine-induced-cardiomyopathy-a-biopsy-proven-case-series/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/hydroxychloroquine-induced-cardiomyopathy-a-biopsy-proven-case-series/