Session Information
Session Type: Abstract Session
Session Time: 12:30PM-12:45PM
Background/Purpose: Forced vital capacity (FVC) is one of the primary disease measures monitored in RA-associated interstitial lung disease (RA-ILD). While prior studies have suggested a minority of RA-ILD patients fulfill a progressive phenotype specified for inclusion in antifibrotic clinical trials, the trajectories of FVC over time in large, real-world RA-ILD populations are not well described. We investigated FVC trajectories among RA-ILD patients within the Veterans Health Administration, the largest integrated healthcare system in the U.S.
Methods: We performed a cohort study of RA-ILD patients within the Veterans Health Administration between 1999 and 2021. RA-ILD patients were identified using validated RA and ILD algorithms ( >80% PPV for RA-ILD), then followed until death or end of study. FVC values were obtained from VA databases of pulmonary function test (PFT) results and also extracted from clinical notes (when primary PFT results were not available) using a validated natural language processing tool. All available FVC values were utilized. Group based trajectory modeling was utilized to derive unique longitudinal trajectories of FVC values, with selection of the optimal numbers of trajectories determined by model fit characteristics (AIC/BIC), group size, and clinical interpretability. Trajectory group membership was used to predict survival and respiratory hospitalization following RA-ILD index date in Cox regression models that included age, sex, race, smoking status, comorbidity burden, and calendar year.
Results: We studied 5,172 RA-ILD patients (92.3% male, mean age 68.8 years) with 18,007 FVC values and identified eight unique FVC trajectories (Figure 1). While initial FVC values were a major determinant of group membership, four of eight trajectory groups (54% of patients) were characterized by a mean FVC % predicted decline >0.7%/year during follow-up (range -0.73 to -1.56%/year). Over 24,780 patient-years of follow-up, 3,400 deaths and 2,763 respiratory hospitalizations occurred. Survival significantly differed across FVC trajectory groups, with trajectory groups characterized by greater FVC decline being associated with poorer survival (adjusted HR 1.56 [1.45-1.67] for groups 3, 5, 7, and 8 combined progressive vs. groups 1, 2, 4, and 6 combined non-progressive) (Figure 2A-B). Progressive trajectory groups were also associated with respiratory hospitalization risk (Figure 3A) with the combined progressive FVC trajectory groups having a >1.6-fold higher risk than the combined non-progressive groups (Figure 3B). Findings persisted when adjusting for baseline FVC (not shown).
Conclusion: Within a large, national RA-ILD population, we identified eight unique trajectories of the RA-ILD disease course characterized by differing patterns of longitudinal FVC values. A progressive RA-ILD disease course (mean decline in FVC % predicted of 0.7 to 1.6 per year) occurred amongst 54% of RA-ILD patients and was predictive of poorer survival and respiratory hospitalization. These findings highlight RA-ILD heterogeneity and the prognostic value of monitoring disease trajectories with longitudinal FVC measurements.
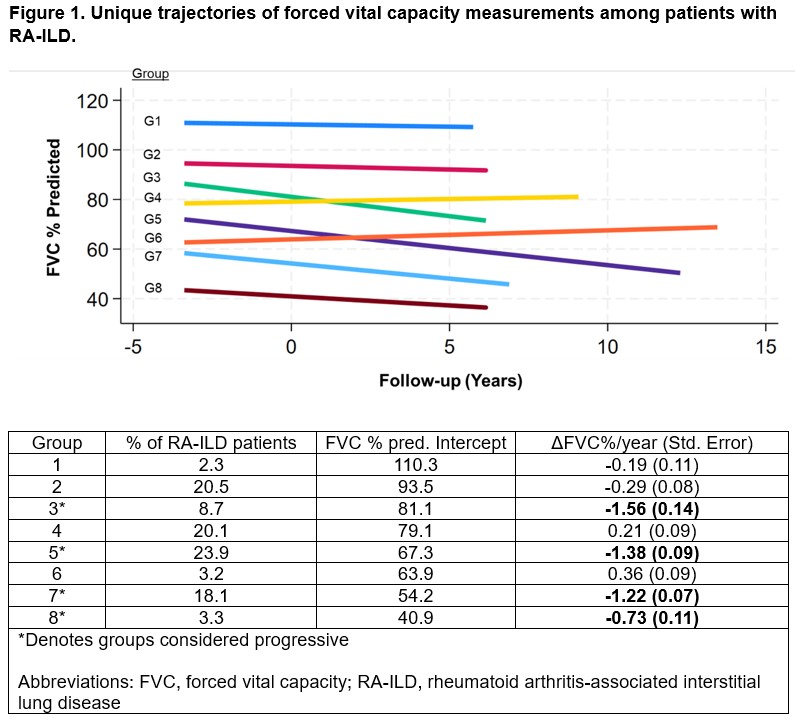 Figure 1. Unique trajectories of forced vital capacity measurements among patients with RA-ILD.
Figure 1. Unique trajectories of forced vital capacity measurements among patients with RA-ILD.
.jpg) Figure 2. Kaplan-Meier curves depicting survival among RA-ILD patients by FVC trajectory group assignment.
Figure 2. Kaplan-Meier curves depicting survival among RA-ILD patients by FVC trajectory group assignment.
.jpg) Figure 3. Kaplan-Meier curves depicting survival free of respiratory hospitalization by forced vital capacity trajectory groups.
Figure 3. Kaplan-Meier curves depicting survival free of respiratory hospitalization by forced vital capacity trajectory groups.
To cite this abstract in AMA style:
England B, Yang Y, Roul P, Johnson T, Matson S, Cannon G, Sauer B, Curtis J, Baker J, Mikuls T. Heterogeneity of RA-ILD by Longitudinal Forced Vital Capacity Measurements Is Associated with Survival and Respiratory Hospitalization [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/heterogeneity-of-ra-ild-by-longitudinal-forced-vital-capacity-measurements-is-associated-with-survival-and-respiratory-hospitalization/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/heterogeneity-of-ra-ild-by-longitudinal-forced-vital-capacity-measurements-is-associated-with-survival-and-respiratory-hospitalization/