Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Cardiac sarcoidosis (CS) is an underdiagnosed condition characterized by the formation of non-caseating granuloma in the myocardium, potentially leading to arrhythmia, acute heart failure, and sudden cardiac death. Early diagnosis of CS is crucial to optimize treatment and delay disease progression. Hemodynamic forces (HDFs) measure the global force exchanged between blood volume and myocardium during cardiac magnetic resonance imaging (CMR), and are a novel noninvasive parameter for detecting early cardiac dysfunction. However, HDFs have not yet been studied in patients with suspected CS.
In this study, we aim to investigate left ventricle (LV) HDFs in suspected CS compared to healthy controls (HC). Additionally, we will evaluate the diagnostic role of HDFs in differentiating between confirmed CS and non-CS patients within the suspected CS group.
Methods: In a single-center study, patients with suspected CS and biopsy-proven sarcoidosis were included and underwent a 1.5T CMR exam. These patients were matched with healthy controls of the same age and sex who also underwent a CMR exam. HDFs were obtained for the entire cohort using advanced post-processing software (Medis Suite). In sarcoidosis patients, cardiac involvement was confirmed using the WASOG (World Association for Sarcoidosis Other Granulomatous diseases) 2014 criteria, which notably include the presence of late gadolinium enhancement (LGE), patchy uptake on cardiac FDG-positron emission tomography, and perfusion defects on cardiac scintigraphy. The performance of HDFs for diagnosing CS among sarcoidosis patient was assessed using a logistic regression model using 3 HDFs parameters: LV systolic peak, LV longitudinal force and LV impulse and adjusted for the presence of LGE.
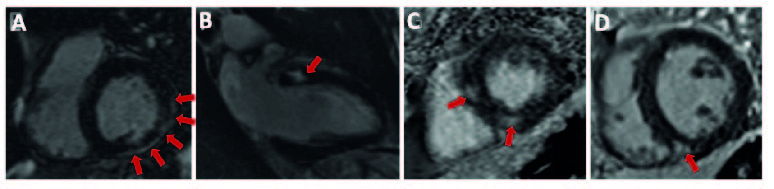
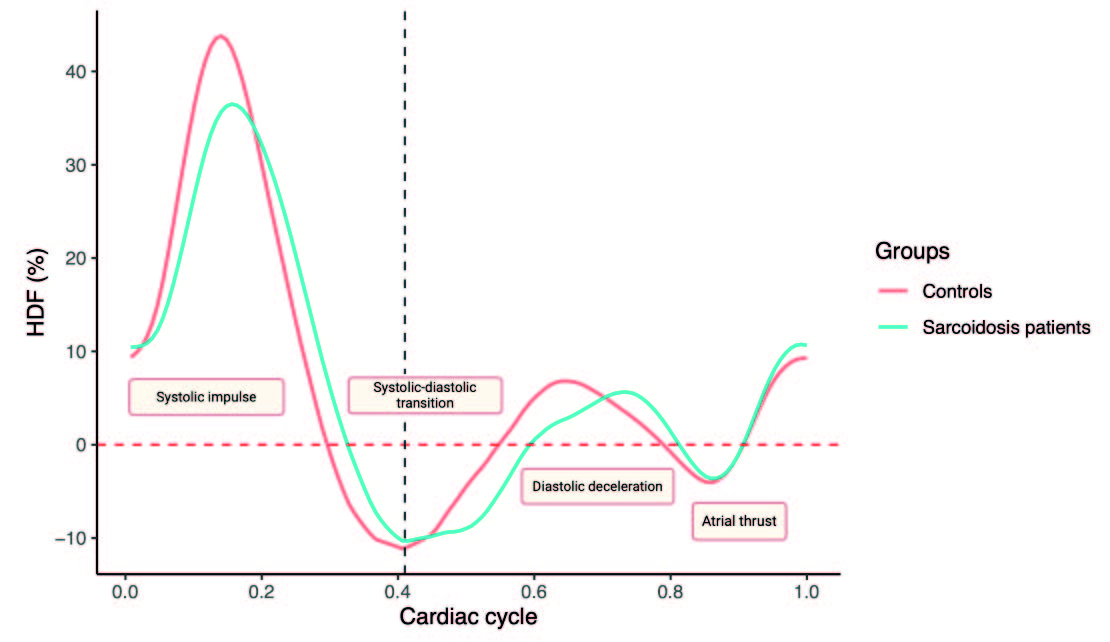
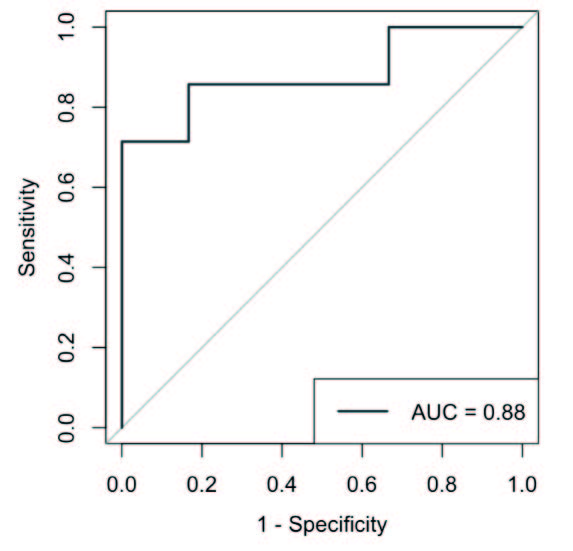
Results: Among 45 sarcoidosis patients with suspected CS, 60% had a confirmed-CS using the WASOG criteria (22% had a positive cardiac FDG-PET, 11% had scintigraphy perfusion defects and 85% had LGE) (Figure 1). In this population, systolic and diastolic HDFs were significantly altered compared to HC (LV impulse, p=0.045; LV systolic ratio, p=0.018; LV systolic-diastolic-transition, p=0.012; LV diastolic deceleration, p=0.013) (Figure 2). In sarcoidosis patients, LV strain and LVEF (median [IQR]) were not statistically different between CS (56 [53–60] %) and non-CS patients (60 [55–64] %). However, HDFs parameters LV longitudinal force (p=0.041), LV impulse (p=0.018), and LV systolic peak (p=0.035) were significantly altered in confirmed-CS patients compared to non-CS patients. Furthermore, the combination of LV longitudinal force, LV impulse, and LV systolic peak enabled an accurate diagnosis of CS among sarcoidosis patients, with an AUROC (area under the receiver operating characteristic) of 0.88 (Figure 3).
Conclusion: Sarcoidosis patients with suspected CS had altered hemodynamic forces compared to HC due to altered LV geometry and mechanics. Furthermore, hemodynamic forces were superior to traditional volumetric and functional CMR parameters (LVEF and strain) to predict cardiac involvement in sarcoidosis patients.
To cite this abstract in AMA style:
Kante A, Afana A, Sène D, Champion K, Pagis V, Bigot W, Delcey V, Lopes A, Tazi A, Amador Borrero B, Crestani B, Baladi C, Bousson V, Goncalves T, Ballout E, Toupin S, mouly s, Dillinger J, Henry P, Pezel T, Comarmond C. Hemodynamic Forces: A Novel Cardiac MRI Parameter to Assess Cardiac Involvement in Sarcoidosis Patients [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/hemodynamic-forces-a-novel-cardiac-mri-parameter-to-assess-cardiac-involvement-in-sarcoidosis-patients/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/hemodynamic-forces-a-novel-cardiac-mri-parameter-to-assess-cardiac-involvement-in-sarcoidosis-patients/