Session Information
Date: Monday, November 13, 2023
Title: (1013–1032) Healthcare Disparities in Rheumatology Poster II: Socioeconomic Determinants
Session Type: Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: Rheumatoid Arthritis (RA) is a chronic autoimmune disease that requires access to subspecialty care. Although Canada has a universal healthcare system, there are complex and interrelated factors that lead to inequitable healthcare access and delivery. These factors are particularly relevant to Canada’s geographically dispersed First Nations People (FN), who bear a disproportionate burden of RA and its complications. In the context of a longitudinal study of RA onset in a FN population, we sought to identify factors that influence access to healthcare in a cohort of FN RA patients and their First-Degree Relatives (FDR).
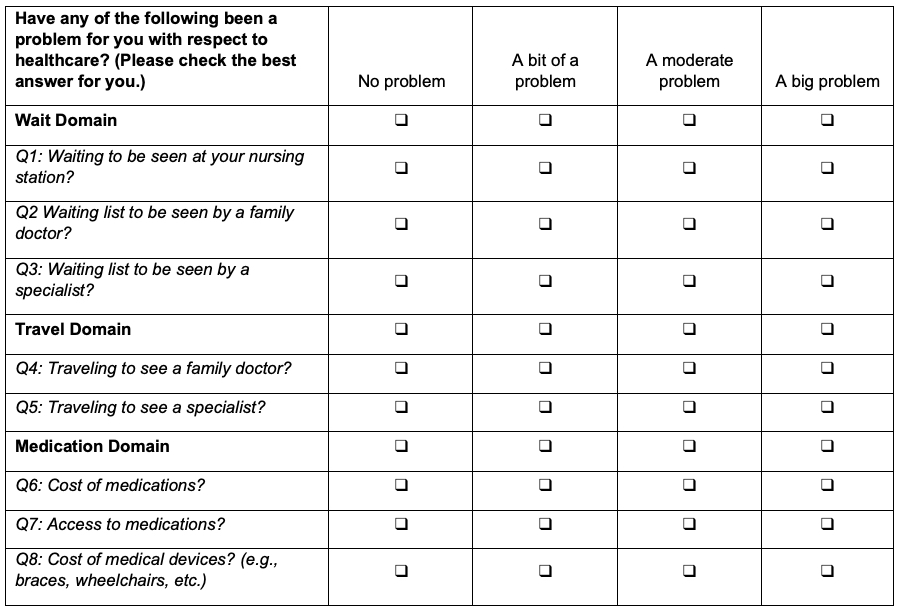
Methods: A longitudinal cohort of FN RA patients (n = 214) and their FDR (n = 617) was recruited between 2005 and 2017 to participate in a prospective study of RA risk in the FDR (total n = 831). Study participants were recruited in both urban and rural locations in Manitoba, Canada. The study enrollment visit included a healthcare access survey which measured access on a Likert scale (Figure 1). Overall access difficulty was determined using a binary variable, where if any of the 7 questions scored moderate or higher, the individual was deemed to have ‘access difficulty’, otherwise they were classified as ‘adequate access’. Modified health assessment questionnaire (mHAQ) and disease duration were collected for RA patients. Data were analyzed using chi-square test and logistic regression.
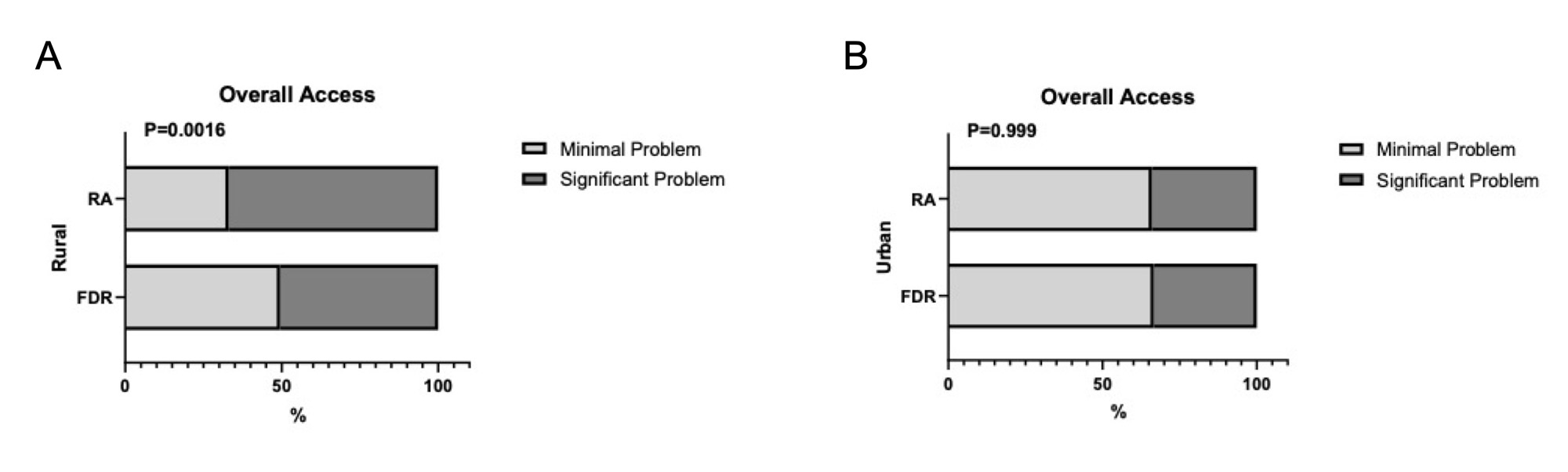
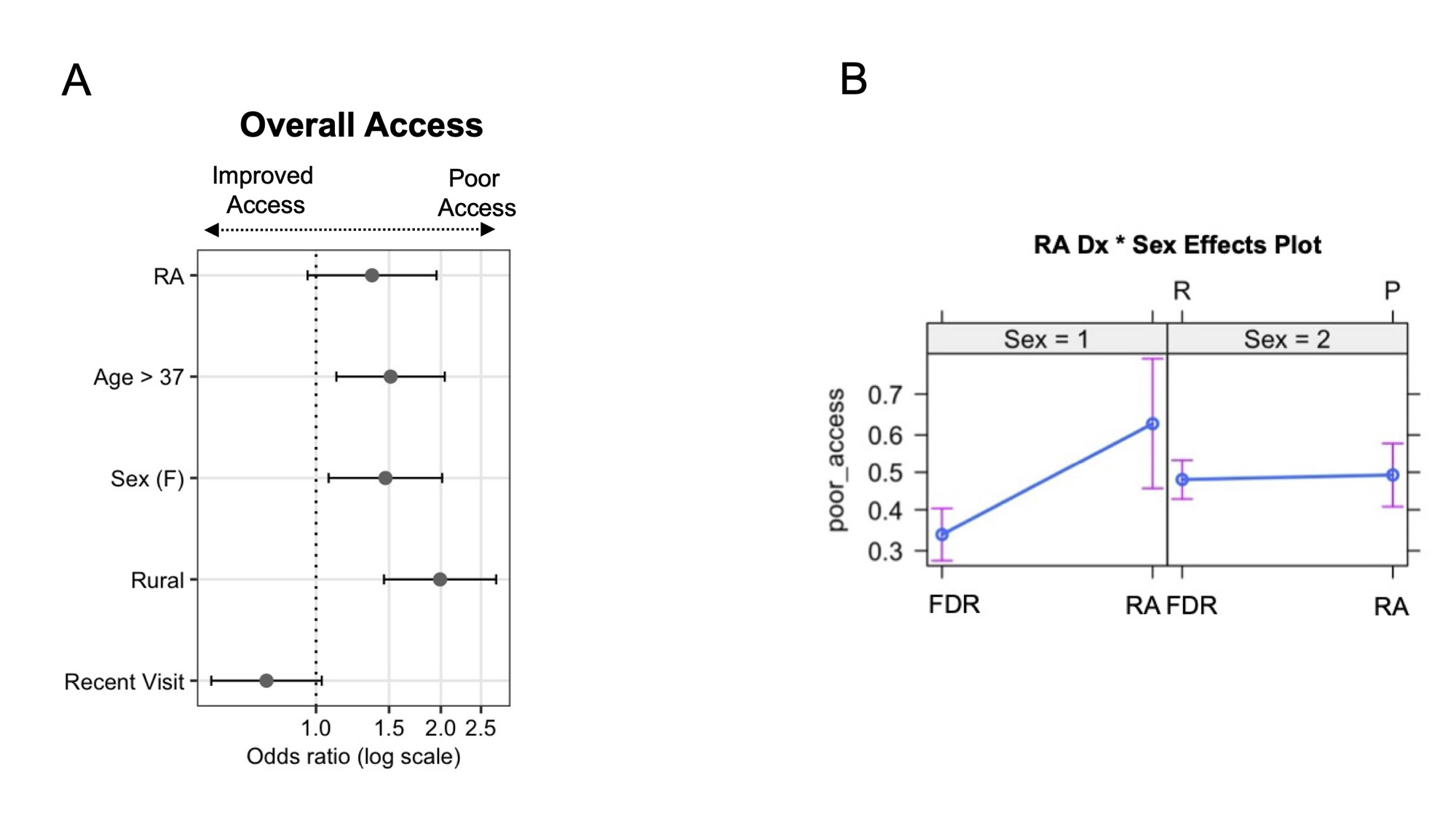
Results: Overall, RA and FDR participants living in rural communities reported more difficulties with healthcare access compared to urban dwellers (overall access difficulty, 53.5% vs 33.5%, p< 0.0001), and rural RA patients reported more access difficulty than unaffected rural FDR (Figure 1A, 66.9% vs 50.5%, p=0.002). In contrast, there were no differences reported between RA patients and FDR living in urban locations (Figure 2B). In the entire RA cohort, no differences in access were reported based on disease duration, age, or sex, although those with higher mHAQ scores tended to report worse access. A logistic regression model of the entire RA and FDR cohort suggested that variables which independently associated with healthcare access difficulty were female sex (Figure 2A, OR 1.47, 1.07-2.01), older age (OR 1.51, 1.12-2.04) and living in a rural community (OR 1.99, 1.45-2.71). The model suggested that females living in rural locations, irrespective of an RA diagnosis, were particularly disadvantaged for healthcare access, but also that males with an RA diagnosis experienced substantially more access difficulty compared to FDR males (Figure 2B).
Conclusion: Perceived difficulties in accessing healthcare were reported more frequently in FN RA patients as well as their unaffected at-risk FDR who were living in rural locations compared to those living in urban locations. We also identified sex, age and location of residence-based differences in perceived healthcare access for FN persons irrespective of disease state. In order to achieve equitable healthcare delivery in the context of a universal healthcare system, interventions to address geographic factors, such as transportation and availability of healthcare providers, need to also incorporate complex factors related to sex, gender and age.
To cite this abstract in AMA style:
Wiens D, Robinson D, Smolik I, Barnabe C, El-Gabalawy H, O'Neil L. Health Care Access in an Indigenous North American Population of Rheumatoid Arthritis Patients and Their At-risk First-Degree Relatives [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/health-care-access-in-an-indigenous-north-american-population-of-rheumatoid-arthritis-patients-and-their-at-risk-first-degree-relatives/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/health-care-access-in-an-indigenous-north-american-population-of-rheumatoid-arthritis-patients-and-their-at-risk-first-degree-relatives/