Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: In the US, health care systems vary, as does cost sharing and access to various RA therapies. However, the burden of RA – a systemic disorder – is often a confounder in management decisions. Whether the burden of RA disease is homogeneous in various regions of the US, and independent of race/ethnicity and/or health care coverage, is unknown.
Methods: US Rheumatology practices from the Northeast, South, and West regions enrolled RA outpatients. Socio-demographics, RA disease status, activity and therapies, and comorbidities were collected, and rheumatic comorbidity disease index (RDCI) was calculated. Primary insurance coverage type (Private, Medicare, Medicaid) was documented, and copay for office visits and medications stratified. Univariable pairwise differences between regions was conducted using Tukey post-hoc corrected analysis of variance for continuous variables, Bonferroni-adjusted Chi-square for categorical variables, and Bonferroni-adjusted logistic regression for dichotomous variables. Multivariable regression models were estimated to investigate disparities in RDCI between insurance variables as well as race while controlling for region.
Results: 402 RA patients were enrolled from 10 outpatient practices (Table). A predominantly Caucasian, female population, with established disease, most received government sponsored primary insurance (40% vs 27.9%). Copay for office visits and medications were < $10 in 45% and 31.8% of observations, respectively, and more prevalent in the Northeast/West subsets than in the South. Office copays > $25 were more frequent in South patients, while more often in Northeast patients for medications. Tobacco use was similar in all subsets. Disease activity scores inclusive of physician/laboratory core measures were higher for South than Northeast patients. RDCI was higher in the South group, 1.7 [1.7], compared to both other subsets and the cohort mean 1.3[1.5]. Hispanics had significantly less RDCI than Blacks (RDCI -0.78, 95% CI [-1.35, -0.21], P=0.008) and Whites (RDCI -0.68, 95% CI [-1.18, -0.17], P=0.009), independent of region. RDCI was significantly lower for privately insured than Medicare (RDCI -0.78, 95% CI [-0.41, -1.15], P< 0.001) and Medicaid (RDCI -0.83, 95% CI [-0.13, -1.54], P=0.020), independent of region. [Figure 1]. However, RDCI was significantly higher for office visit copays < $10 than $25-50 (RDCI +0.61, 95% CI [0.16, 1.06], P=0.008) and $50+ (RDCI +0.89, 95% CI [0.17, 1.62], P=0.016), as well as for medication copays both < $10 (RDCI +0.58, 95% CI [0.12, 1.03], P=0.013) and $10-25 (RDCI +0.67, 95% CI [0.03, 1.31], P=0.041) compared to $25-50, both independent of region. [Figure 2].
Conclusion: While RA disease burden was evident in patients receiving care in Southern practices, it was independent of race/ethnicity. Government health care rather than private insurance plans covered complicated RA patients, regardless of site of care. Cost sharing may further complicate access to optimum care. Application of this analysis to a larger dataset that includes additional US regions, expanded insurance parameters and potential founders such as socioeconomic status, is needed.
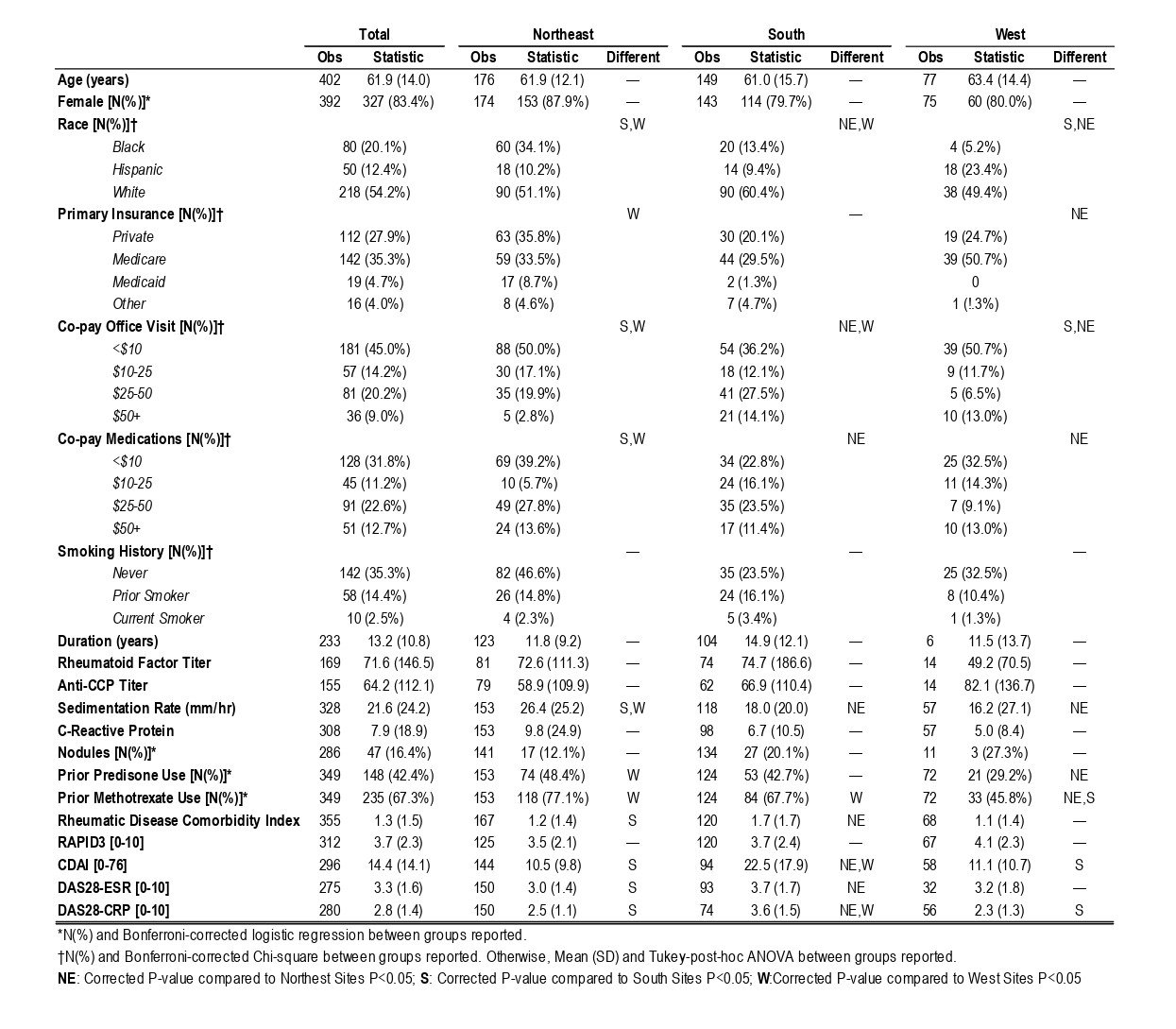 Table: Clinical Characteristics of RA patients in US Geographic Regions
Table: Clinical Characteristics of RA patients in US Geographic Regions
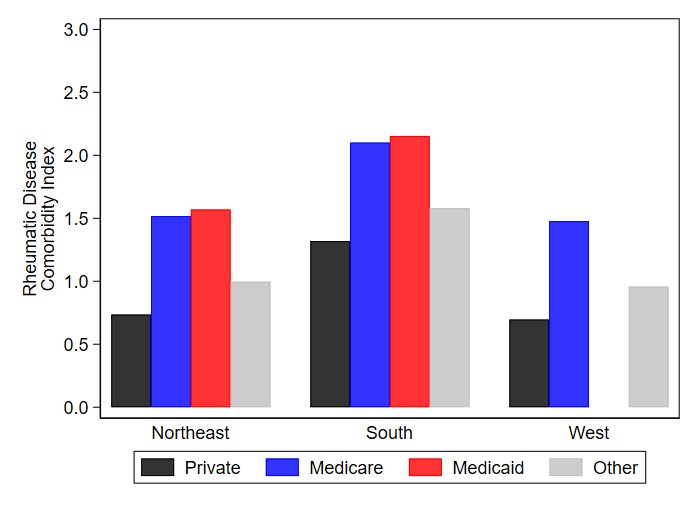 Figure 1. Rheumatic Disease Comorbidity Index by Region and Insurance Type
Figure 1. Rheumatic Disease Comorbidity Index by Region and Insurance Type
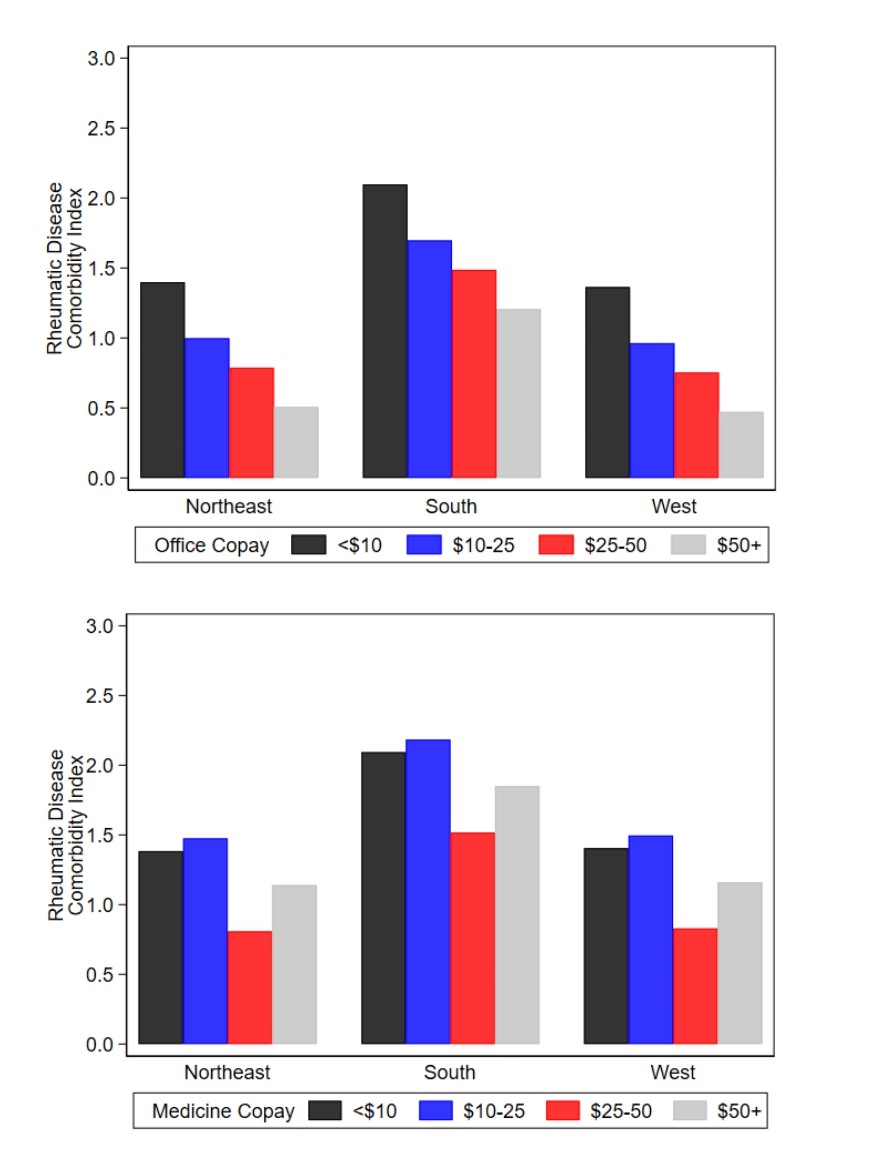 Figure 2. Rheumatic Disease Comorbidity Index by Region and Office and Medication Co-pay
Figure 2. Rheumatic Disease Comorbidity Index by Region and Office and Medication Co-pay
To cite this abstract in AMA style:
Kerr G, Swearingen C, Pedra-Nobre M, Wollaston D, Najmey S, Lawrence-Elliott C, Lawrence Ford T, Dowell S, North H, Dore R, Dolatabadi S, Ramanujam T, Winkler A, Kennedy S, Jileaeva I, Richardson A, Kaine J, Wright G. Geographical Disparity in Rheumatoid Arthritis Disease Burden Independent of Race/Ethnicity [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/geographical-disparity-in-rheumatoid-arthritis-disease-burden-independent-of-race-ethnicity/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/geographical-disparity-in-rheumatoid-arthritis-disease-burden-independent-of-race-ethnicity/