Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Gender and ethnic disparities in health care are well reported in the general medical literature. Differences in symptom reporting or perceived health status can affect provider’s treatment recommendation. Specific to rheumatoid arthritis (RA), RAPID-3 (R3) is a validated RA-specific questionnaire that assesses symptom severity and disease burden. Our primary objective was to assess gender and ethnic disparities in perceived disease burden as measured by R3. Our secondary objective was to determine the strength of association between R3 against the gold standard of RA disease activity, the Clinical Disease Activity Index (CDAI) that requires a joint examination.
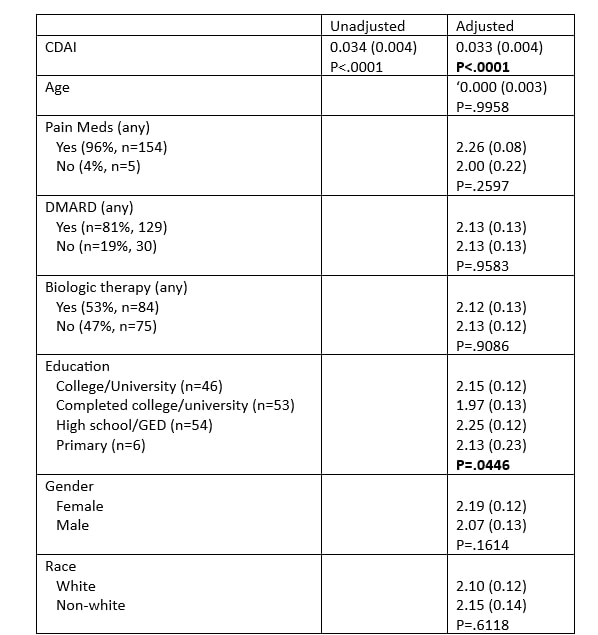
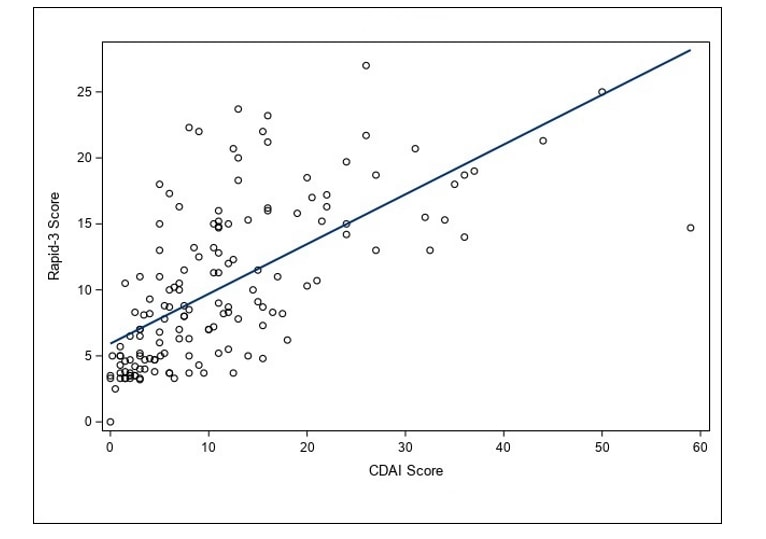
Methods: We recruited 159 patients with RA in an academic rheumatology practice. In the analyses, the primary dependent variable was R3 and the primary independent variables were gender and race. Using generalized linear models, analyses were controlled for the following covariates: age, pain medications, use of DMARD, biologic therapy, education and CDAI. Further, the association of CDAI and R3 was assessed with Spearman non-parametric correlation analyses.
Results: The sample (n= 159) cohort had the following traits: a mean age 61 (SD 12.9); 62% (n=99) with college degree, 73% of whom were females; 15.7% (n=25) African American, 77% (n=123) White, and 4.4% (n=7) other; 96.9% were on pain medications, 81.1% on DMARD therapy, and 52.8% on biologics. On bivariate analyses, gender and race were not associated with R3. After controlling for potential confounders, race and gender remained non-significant. None of the covariates was associated with R3, except for CDAI and education. Specifically, compared to those with high school diploma/GED, those who completed college reported higher R3 scores. Importantly, CDAI was strongly associated with R3. Figure 1 shows moderate linear relationship between CDAI and RAPID 3 (R2= 0.42 and p< 0.001).
Conclusion: We found no gender or ethnic differences in perceived disease burden as measured by R3. R3 was moderately associated with CDAI; and thus, can be used as a tool to assess RA disease activity. In today’s world of telehealth medicine, rheumatology providers can rely on a subjective measure like R3 to assess RA disease activity. Our findings cannot be generalized to RA patients with coexisting fibromyalgia.
To cite this abstract in AMA style:
Malik A, Ang D, Hall A, Herion J, Thapa R. Gender and Ethnic Differences (or Lack Thereof) in Perceived Disease Burden in RA [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/gender-and-ethnic-differences-or-lack-thereof-in-perceived-disease-burden-in-ra/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/gender-and-ethnic-differences-or-lack-thereof-in-perceived-disease-burden-in-ra/