Session Information
Date: Monday, November 11, 2019
Title: 4M097: Systemic Sclerosis & Related Disorder – Clinical II: Cardiopulmonary Involvement (1830–1835)
Session Type: ACR Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Pulmonary fibrosis (PF) is common in systemic sclerosis (SSc) and serial pulmonary function tests (PFTs) are used for routine PF monitoring. Forced vital capacity (FVC) decline reflects progression in PF and FVC is frequently used as an endpoint in clinical trials assessing the effect of drugs on PF. We explore the changes in FVC over time in a cohort of patients with SSc-related PF receiving standard management, including immunosuppression.
Methods: Only SSc patients with CT-confirmed PF were included. FVC changes over the first 10 years from disease onset and the effects of age, sex, cutaneous subset and autoantibodies were assessed using linear mixed effect models. We analysed time to development of threshold FVC levels (FVC< 70% and FVC< 50%) on a time scale starting at first available FVC, if this was within the first 5 years of disease, using Kaplan-Meier estimates and Cox regression.
Results: From a single centre cohort of 1068 SSc patients with at least one PFT result available, we identified 505 (47.3%) who had PF. Of those 109 (21.6%) were male, average age of onset was 47 years and 249 (49.3%) had diffuse cutaneous subset (dcSSc). The most common autoantibody was anti-topoisomerase I (ATA) in 204 (40.4%) of the subjects, followed by anti-RNA polymerase in 59 (11.7%), anti-PmScl in 26 (5.2%), anti-centromere in 36 (7.1%) and anti-U3RNP in 15 (3.0%). In 83 (16.4%) of the patients ANA was positive, but no ENAs were identified (ANA+ENA-). FVC measurements on at least three occasions were available for 364 (72.1%) of the patients. Mean period between PFTs was 13 months.
Average FVC at 12 months from onset was 80.1% (SD 19.3). For most patients, FVC fluctuated over time, although there was a small but statistically significant absolute decline of approximately 0.32% per year (95%CI 0.09, 0.55; p=0.007) at a group level. There was no evidence for a significant correlation between baseline FVC and subsequent change (correlation coefficient -0.13, 95%CI -0.26, 0.01). Multivariable analysis demonstrated significant associations between FVC and age at onset, sex, cutaneous subset and antibodies (Table 1).
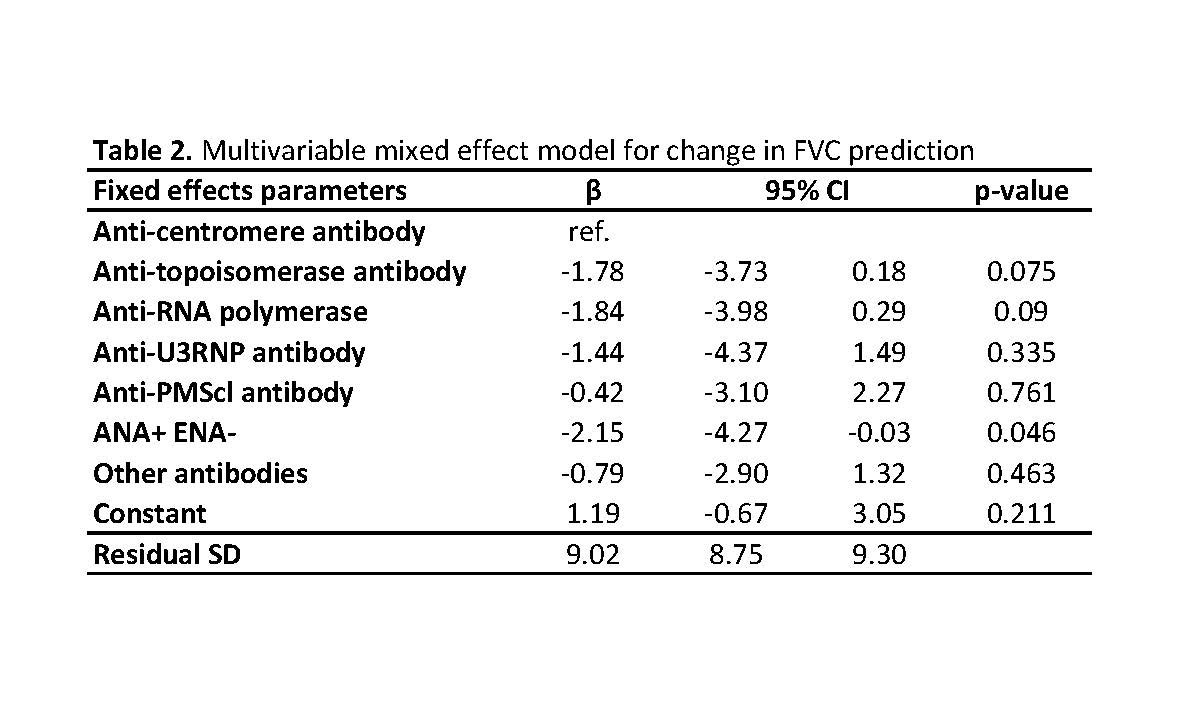
In a multivariable model for change in FVC (difference between FVC measured in consecutive PFTs), only antibodies predicted future change with greatest drop observed in ANA+ENA- patients, followed by ARA+ and ATA+ ones (Table 2).
The proportion of PF subjects to develop FVC< 70%, if they had FVC≥70% at first available test, was 7.7% at 1 year, 13.6% at 2 years, 17.2% at 3 years, 18.7% at 4 years and 19.8% at 5 years from first FVC assessment. For FVC< 50% this was 2.1% at 1 year, 4.4% at 2 years, 5.8% at 3 years, 7.6% at 4 years and 10.5% at 5 years. In a multivariable model, factors that associated with increased risk for FVC drop below 70% were male sex, ATA positivity and low baseline FVC, while the only predictor of drop in FVC to 50% or lower was low baseline FVC (Table 3).
Conclusion: This study provides insight into long-term patterns of FVC change and develops a model that may help predict those most at risk of significant decline. We show that ATA positivity, male gender and diffuse subset are associated with greater long-term decline in FVC, while short-term change associated only with antibodies.
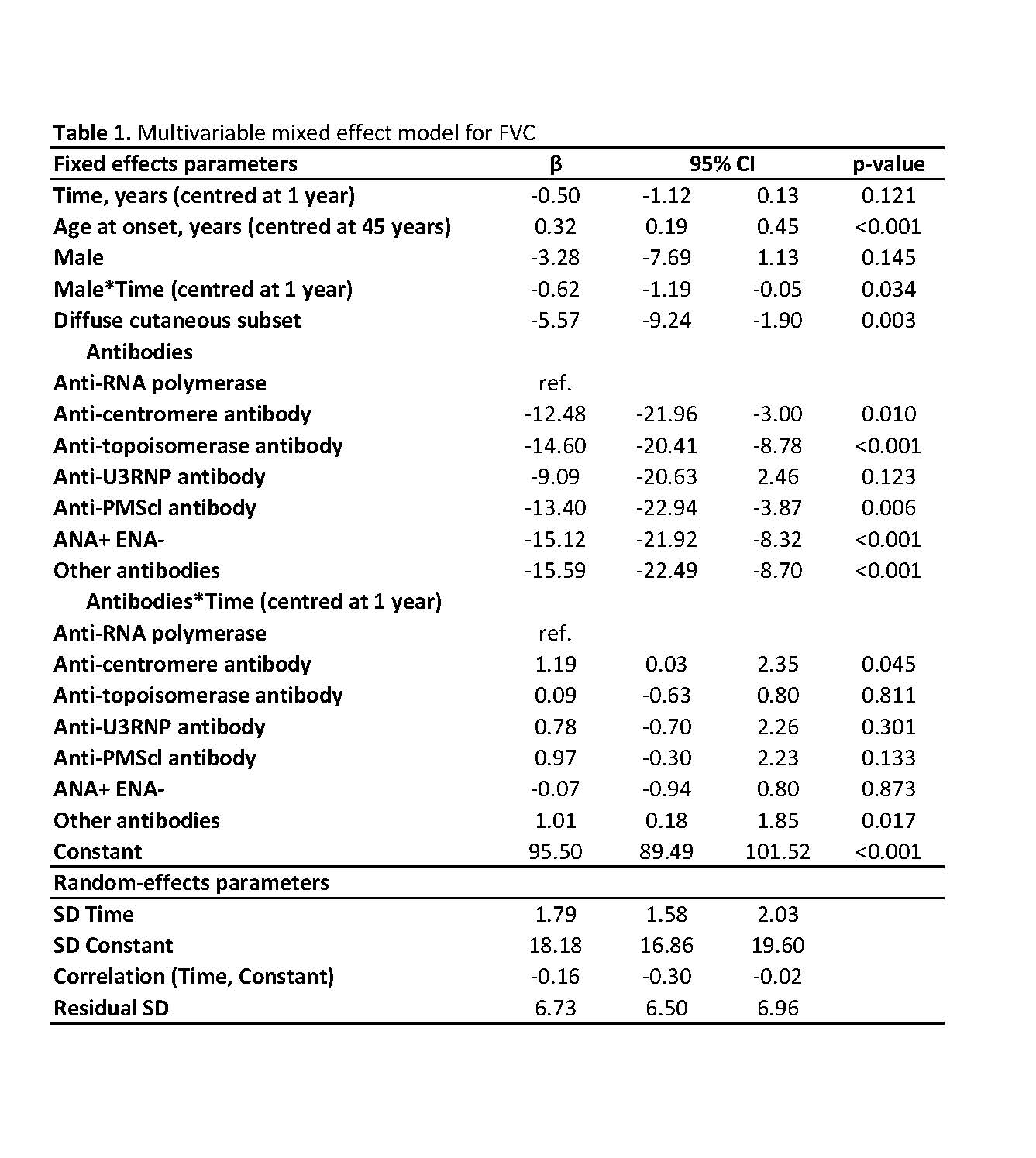
ACR_2019_Lung_Table1
ACR_2019_Lung_Table2

ACR_2019_Lung_Table3
To cite this abstract in AMA style:
Nihtyanova S, Derrett-Smith E, Fonseca C, Ong V, Denton C. Frequency and Predictors of Meaningful Decline in Forced Vital Capacity During Follow up оf a Large Cohort of Systemic Sclerosis Associated Pulmonary Fibrosis Patients [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/frequency-and-predictors-of-meaningful-decline-in-forced-vital-capacity-during-follow-up-%d0%bef-a-large-cohort-of-systemic-sclerosis-associated-pulmonary-fibrosis-patients/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/frequency-and-predictors-of-meaningful-decline-in-forced-vital-capacity-during-follow-up-%d0%bef-a-large-cohort-of-systemic-sclerosis-associated-pulmonary-fibrosis-patients/