Session Information
Date: Monday, November 14, 2022
Title: Abstracts: RA – Diagnosis, Manifestations, and Outcomes II: Cardiovascular and Other Comorbidities
Session Type: Abstract Session
Session Time: 9:00AM-10:30AM
Background/Purpose: Rheumatoid arthritis (RA) is known to cause increased risk of cardiovascular (CV) disease (CVD) due to the underlying inflammation. The year of 2010 revolutionised the clinical landscape of RA with the updated classification criteria allowing earlier classification of RA and with the recommendation of the treat-to-target (T2T) treatment approach. It is uncertain if the excess CVD risk could be ameliorated by effective suppression of inflammation using the T2T approach in patients with early RA (ERA). This study compared the incidence of CVD among ERA patients managed by a T2T strategy with a CV risk factor-matched non-RA population and a historical RA cohort (HRA).
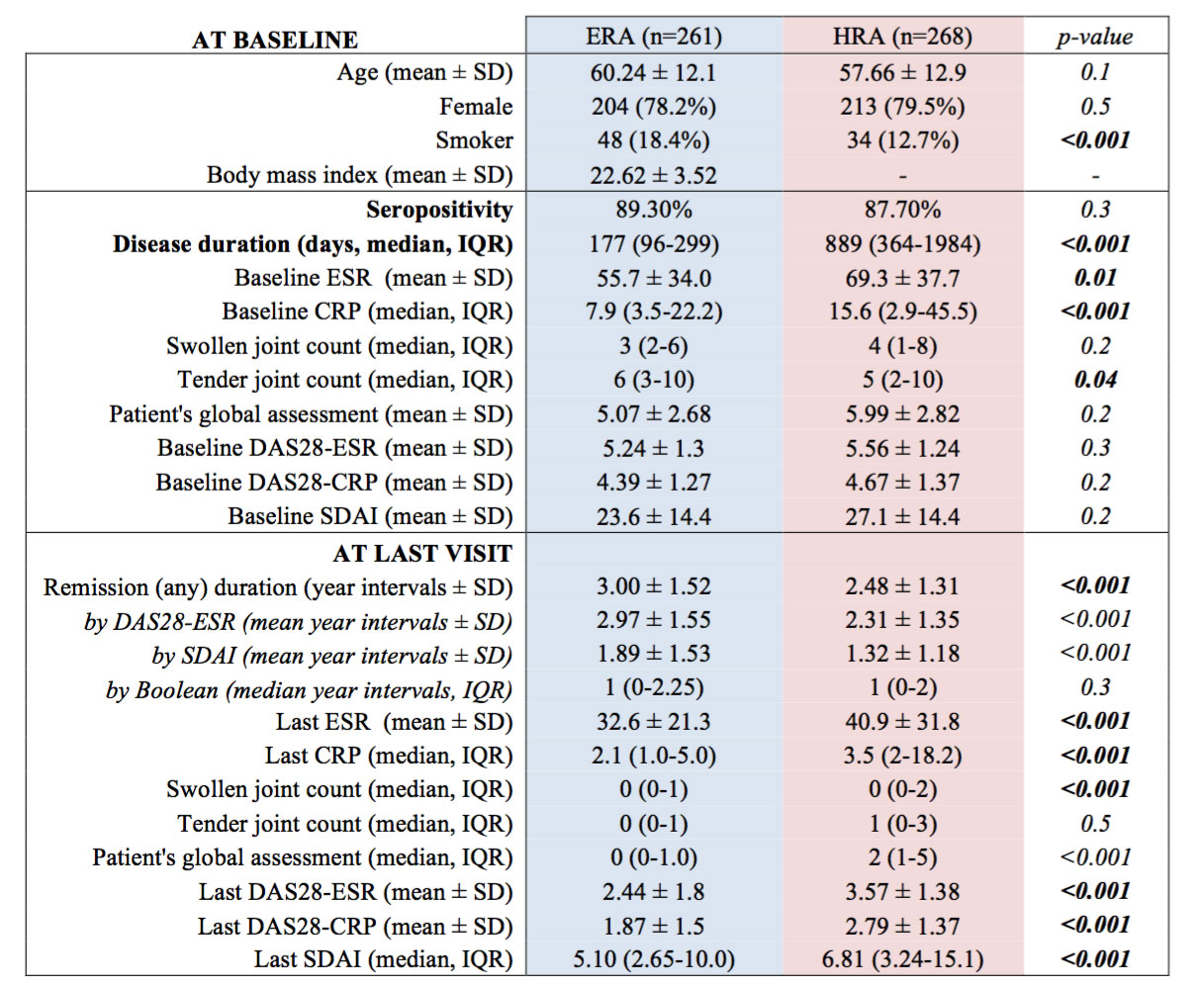
Methods: This was an observational study using the territory-wide electronic health record system of Clinical Data Analysis and Reporting System (CDARS) and the Clinical Rheumatology Systemic Treat-to-target in Asia Leadership (CRYSTAL) registry. Two hundred and sixty-one ERA patients diagnosed between 2012-2016 with baseline disease duration less than 2 years were recruited. A HRA cohort with 268 RA patients diagnosed between 2002-2006 was also recruited. All of the ERA patients received T2T management aiming at remission while HRA patients received routine care. Each ERA/ HRA patient was matched to 3 non-RA controls according to age, gender, smoking status and CV risk factors including the presence of diabetes mellitus, hypertension and hyperlipidaemia. All subjects on antiplatelet/ anticoagulant agents, with pre-existing CVD, chronic kidney disease or other autoimmune diseases at baseline were excluded. All subjects were followed until death, migration or up to 5 years from baseline. Data of RA-related clinical and laboratory parameters were comprehensively collected at baseline and then at least annually. The primary endpoint was the first occurrence of a CV event (CVE). Secondary outcomes were the comparison of CVE incidence between different cohorts, differences in the inflammatory burden and treatment used between the ERA and HRA cohorts, and the RA-specific factors (inflammation and treatment) for predicting CVE among all RA patients.
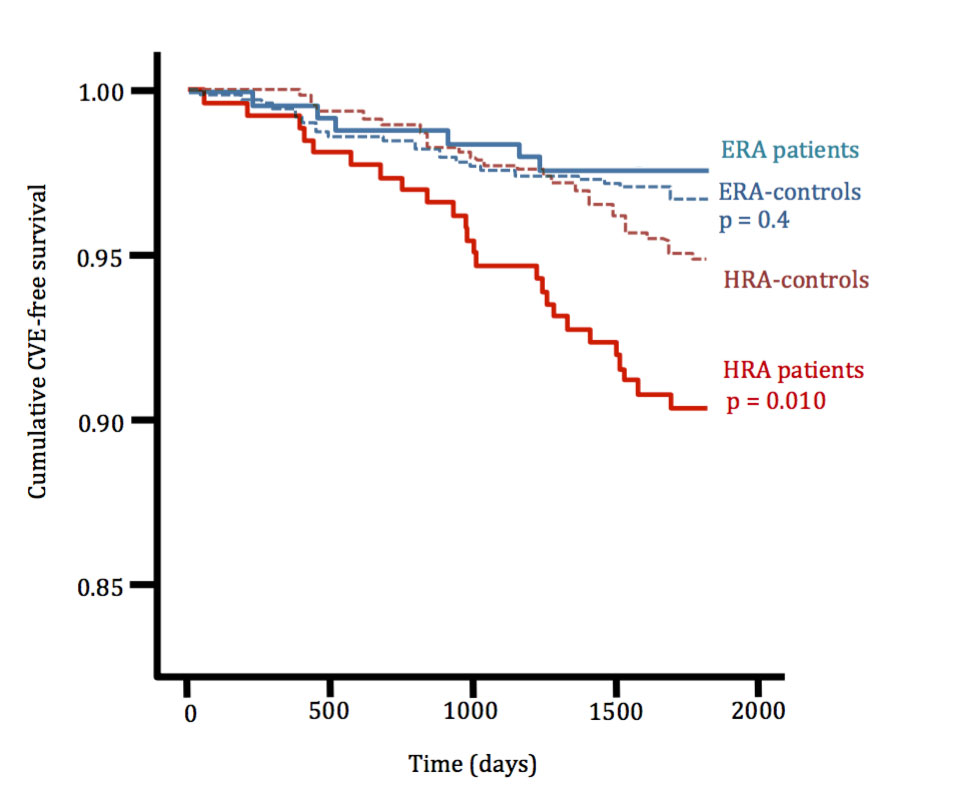
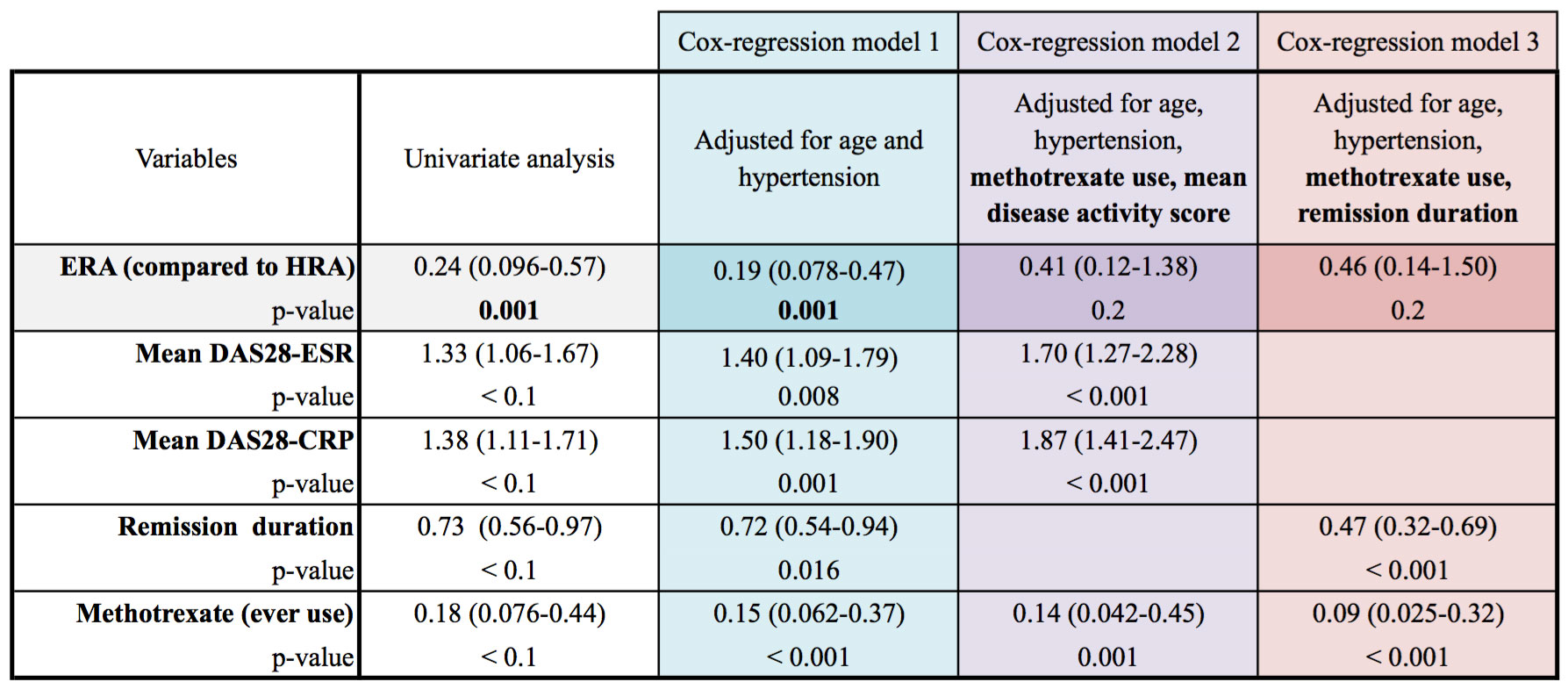
Results: A total of 261 ERA patients, 783 ERA-controls, 268 HRA patients and 804 HRA-controls were eligible for this study. The incidence of CVE among ERA cohort & ERA-controls were similar (4.6 and 6.6 per 1000 persons-year respectively), with an unadjusted hazard ratio of 0.53 (95% confidence interval [CI] 0.15-1.79). In contrast, the incidence of CVE in HRA cohort was significantly higher than that of the HRA-controls with an unadjusted hazard ratio of 1.9 (95% CI 1.16-3.13). The incidence of CVE in the ERA cohort was significantly lower than that of the HRA cohort with an unadjusted hazard ratio of 0.24 (95% CI 0.1-0.6); the difference became insignificant after adjusting for inflammation (mean disease activity or remission duration), the use of methotrexate and traditional CV risk factors.
Conclusion: ERA patients managed by a T2T strategy did not develop excess CVE compared to CV risk factor-matched controls over 5 years. This diminished CVE risk among ERA patients could be explained by the lower mean disease activity, longer remission duration and the use of methotrexate.
To cite this abstract in AMA style:
Tam L, Lam T, Wan M. Five-Year Cardiovascular Event Risk in Early Rheumatoid Arthritis Patients Who Received Treat-to-Target Management [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/five-year-cardiovascular-event-risk-in-early-rheumatoid-arthritis-patients-who-received-treat-to-target-management/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/five-year-cardiovascular-event-risk-in-early-rheumatoid-arthritis-patients-who-received-treat-to-target-management/