Session Information
Date: Tuesday, November 14, 2023
Title: (2387–2424) Vasculitis – Non-ANCA-Associated & Related Disorders Poster III
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Steroids and anti-IL6 biotherapy are highly effective in obtaining remission in patients with giant cell arteritis (GCA) but the risk of relapses remains high, especially once treatments are withdrawn. Predictors of relapse in GCA are missing. We aimed to identify predictors of relapse in GCA.
Methods: All consecutive patients admitted with a new diagnosis of GCA in our national center for rare immune-mediated inflammatory diseases (Bichat hospital, Paris, France) between January 2011 to December 2021 were eligible for this study. Patients were included if the 2022 American College of Rheumatology/EULAR classification criteria for GCA were met. GCA relapse was defined by the presence of recurrent or new-onset disease related symptoms, an increase of CRP value >10mg/L and the necessity for an increase in the prednisone dose. The primary outcome was the GCA relapse rate over the 36-months follow up. Factors associated with the primary outcome were identified and time to first relapse was studied with a multivariable Cox model.
Results: One hundred and eight patients (74 [69-81] years, 65% of women) with a new diagnosis of GCA were studied. At diagnosis, 87 (81%) patients had cranial symptoms. CRP was high ( > 10 mg/L) in all but 5 cases (90%) with a median level of 64 [34-132] mg/L. GCA was biopsy-proven in 65 (64%) cases. Ninety-eight (91%) FDG/PET CT performed at diagnosis were available for a systematic review of FDG uptake in aorta, supra-aortic trunks, and limb (axillary and iliofemoral) arteries. Unequivocally strong linear large vessels wall FDG uptake was found in 74 (73%) cases. All patients received steroids given for 21.0 [18.0-28.5] months, associated with methotrexate or tocilizumab in 1 (1%) and 2 (2%) cases, respectively. During a median follow-up of 27.5 [11.4 – 35.0] months, 40 (37%) patients experienced GCA relapse. Univariate analysis showed that FDG uptake in limb arterie sat diagnosis was associated with GCA relapse: relapse occurred in 58% (n=14/24) of patients with FDG uptake in limb arteries and in 28% (n=21/74) of patients without FDG uptake in limb arteries(p=0.008). Multivariable Cox regression model, including age, gender, thickened aortic wall, FDG uptake in limb arteries and IV steroid pulse as covariates, showed that FDG uptake in limb arterie sat diagnosis was the unique identified risk factor for relapse (HR 3.05 [1.48-6.25], p=0.002) (Figure 1).
Conclusion: FDG uptake in limb arteries at diagnosis of GCA is associated with relapse. FDG/PET CT may help to better tailor therapy in GCA.
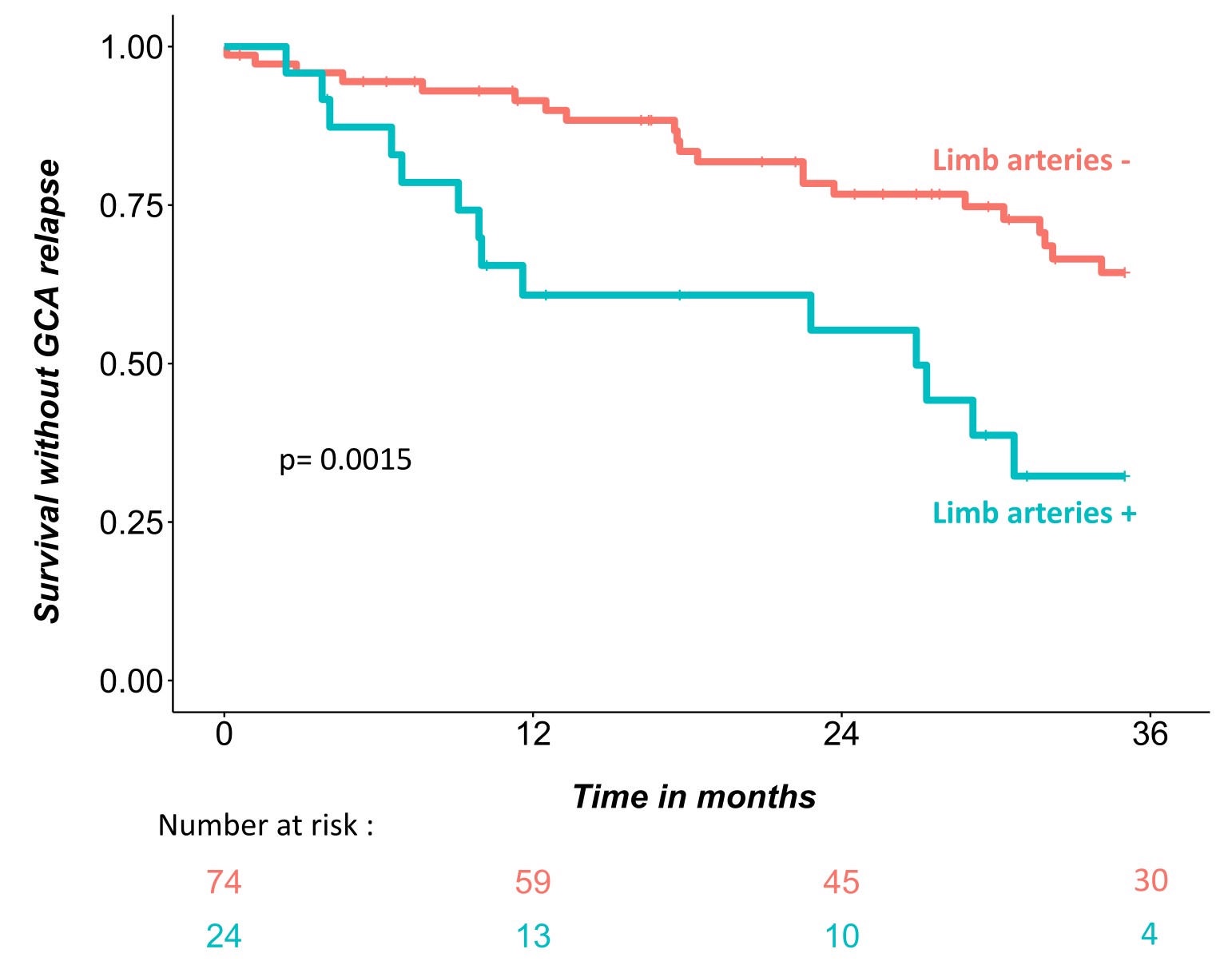
Patients with FDG uptake in limb arteries (limb arteries +) at diagnosis had higher rates of relapse than patients without FDG uptake in limb arteries (limb arteries -) at diagnosis (log-rank; p = 0.0015).
To cite this abstract in AMA style:
Peyrac G, Mageau A, Gaudemer A, Benali K, Alexandra J, Strukov A, Ottaviani S, Papo T, Sacre K. FDG Uptake in Limb Arteries at Diagnosis of Giant Cell Arteritis and Risk of Relapse: An Observational Cohort Study [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/fdg-uptake-in-limb-arteries-at-diagnosis-of-giant-cell-arteritis-and-risk-of-relapse-an-observational-cohort-study/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/fdg-uptake-in-limb-arteries-at-diagnosis-of-giant-cell-arteritis-and-risk-of-relapse-an-observational-cohort-study/