Session Information
Date: Monday, November 8, 2021
Session Type: Poster Session C
Session Time: 8:30AM-10:30AM
Background/Purpose: Psoriasis, a chronic immune-mediated skin disease affecting 2-4% of the US population, is increasingly recognized as a systemic inflammatory disorder associated with cardiometabolic and other comorbidities. Additionally, psoriasis frequently precedes the development of psoriatic arthritis (PsA) and among patients with psoriasis, certain comorbidities may be risk factors for development of PsA. The objectives of this study were to: 1) investigate the prevalence of comorbidities in an incident cohort of psoriasis patients compared to age- and sex-matched controls, and 2) compare the prevalence of comorbidities in mild psoriasis with moderate to severe psoriasis at diagnosis.
Methods: A population-based incidence cohort of psoriasis subjects ≥18 years of age and first diagnosed between 2000 and 2010 was identified. Complete medical records of all potential psoriasis subjects were reviewed, and psoriasis was defined as a confirmatory diagnosis in the medical record, either by a dermatologist or a physician’s description of the lesions, or a skin biopsy if available. In doubtful cases, medical records were reviewed by a dermatologist. Severity of psoriasis was defined based on the body surface area involved, sites involved, and requirement for phototherapy or systemic therapy. Incident psoriasis cases were age-, and sex-matched to subjects from the same population. Diagnosis codes (≥2 codes at least 30 days apart) within a five-year lookback period were used to determine the presence of comorbidities; at least one year of available medical history was required. Comorbidities were defined using 44 categories (England et al. Ann Rheum Dis. 2021). Standardized differences were calculated to examine differences between psoriasis and controls, and between mild and moderate to severe psoriasis subjects.
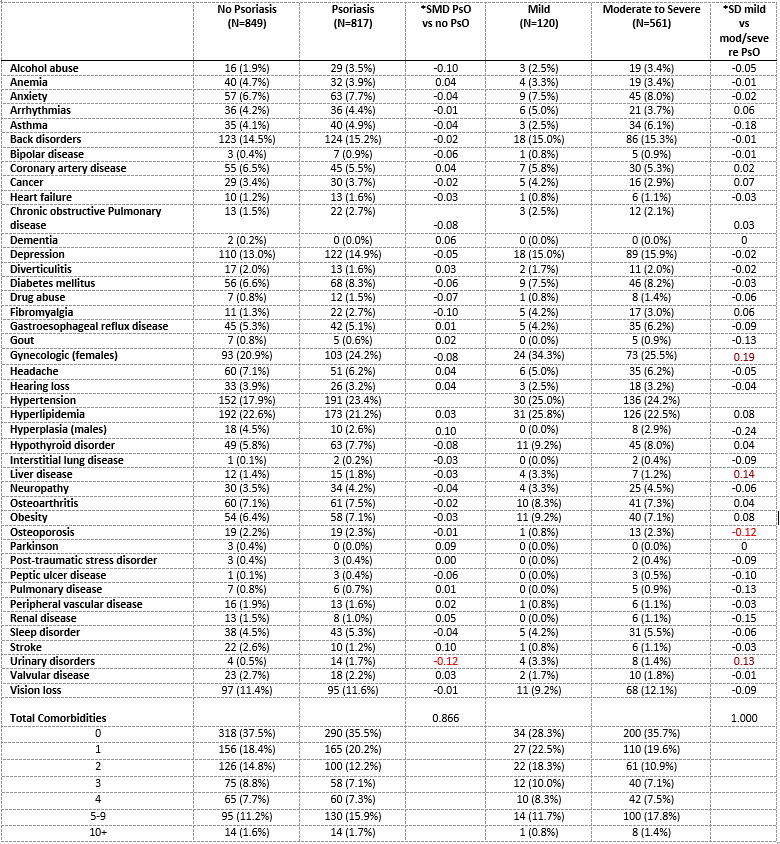
Results: There were 871 incident cases of psoriasis from 2000-2010. Excluding those with < 1 year of prior medical history, 817 psoriasis patients were analyzed, with a mean age of 45.7(SD=16.9) years and 52% females; severity of psoriasis ranking was available for 681 (83.4%). At incidence, 35.5, 20.2, 12.2, 7.1, 7.3, 15.9, and 1.7% of the psoriasis patients had 0, 1, 2, 3, 4, 5-9, and ≥10 England comorbidities. There was no substantial difference in the prevalence of the comorbidities between newly diagnosed psoriasis patients and controls (Table). Similarly, few comorbidities were meaningfully different (SMD >0.1) among subjects with mild psoriasis at diagnosis compared to those with moderate to severe psoriasis at diagnosis (Table).
Conclusion: In this population-based cohort of incident psoriasis, there were no substantial differences in the prevalence of comorbidities (including cardiometabolic) between newly diagnosed psoriasis and the general population. Comorbidities may develop over the course of psoriatic disease with no apparent differences at psoriasis diagnosis. Further studies to examine the trajectory of comorbidities in this incident psoriasis cohort are planned.
To cite this abstract in AMA style:
Karmacharya P, Chakradhar R, Ogdie A, Davis J, Wright K, Tollefson M, Duarte-Garcia A, Bekele D, Maradit Kremers H, Ernste F, Gunderson T, Hulshizer C, Crowson C. Epidemiology of Comorbidities in an Incident Psoriasis Cohort: A Population-Based Study [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/epidemiology-of-comorbidities-in-an-incident-psoriasis-cohort-a-population-based-study/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/epidemiology-of-comorbidities-in-an-incident-psoriasis-cohort-a-population-based-study/