Session Information
Date: Sunday, November 8, 2020
Title: Epidemiology & Public Health Poster III: Inflammatory Rheumatic Disease
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: ANCA-associated vasculitis has a reported prevalence ranging from 3.2 to 9.1 cases per 100,000 individuals, but little is known of geographic variations. The aim of this study is to observe the prevalence of AAV in a rural based health system using updated ACR/EULAR Diagnostic and Classification Criteria for Primary Systemic Vasculitis (DCVAS). The study also provides geographic mapping of cases to investigate potential environmental factors.
Methods: We reviewed patients with potential AAV through use of EHR from 1/1/2003-6/30/2018 with ICD 9/10 codes consistent with AAV, granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), or eosinophilic granulomatosis with polyangiitis (EGPA). We conducted a manual chart review of cases that satisfy ACR/EULAR DCVAS. Each case was independently confirmed by a rheumatologist, pulmonologist and nephrologist. The denominator for a 5-year point prevalence estimate was calculated by identifying patients > 18 years old with a PCP encounter between 1/1/2003-6/30/2018 who had at least one outpatient encounter between 1/1/2014-12/31/2018. The numerator was calculated by identifying AAV cases within the denominator population. The prevalence estimate was calculated using a simple binomial proportion and the simple asymptotic continuity corrected 95% confidence interval. Prevalence estimates for GPA, MPA, and EGPA were calculated using similar methods as for overall AAV prevalence. Because of the rarity, the 95% confidence interval for the EGPA is reported using a Clopper-Pearson exact method. Statistical analysis was completed using SAS 9.4. All confirmed cases of AAV were plotted along a map to evaluate geographic distribution.
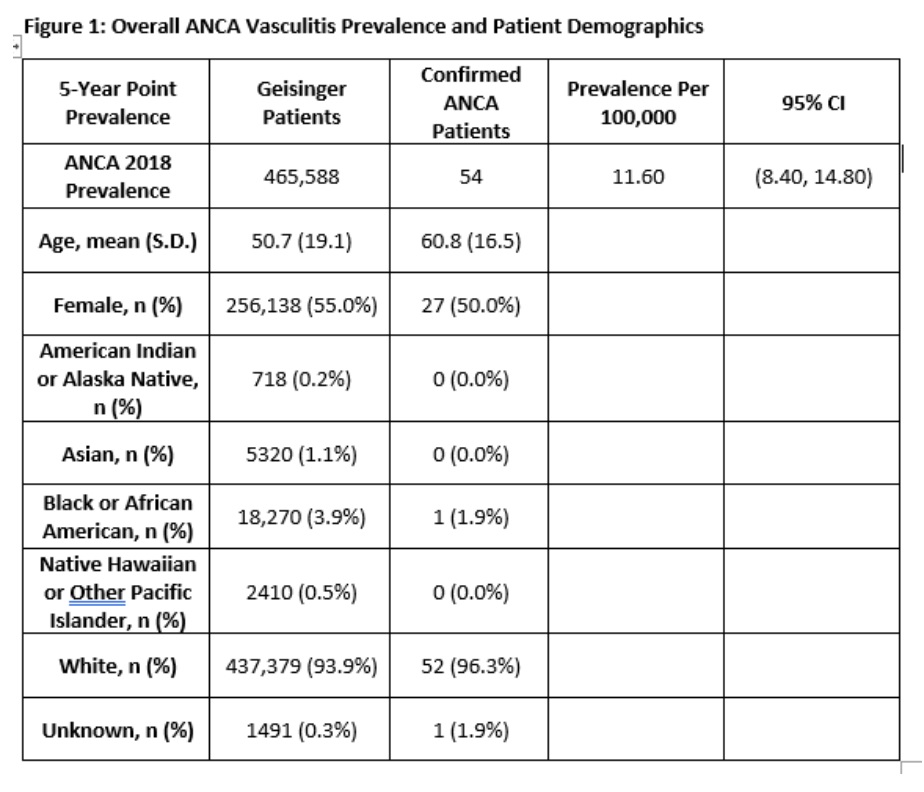
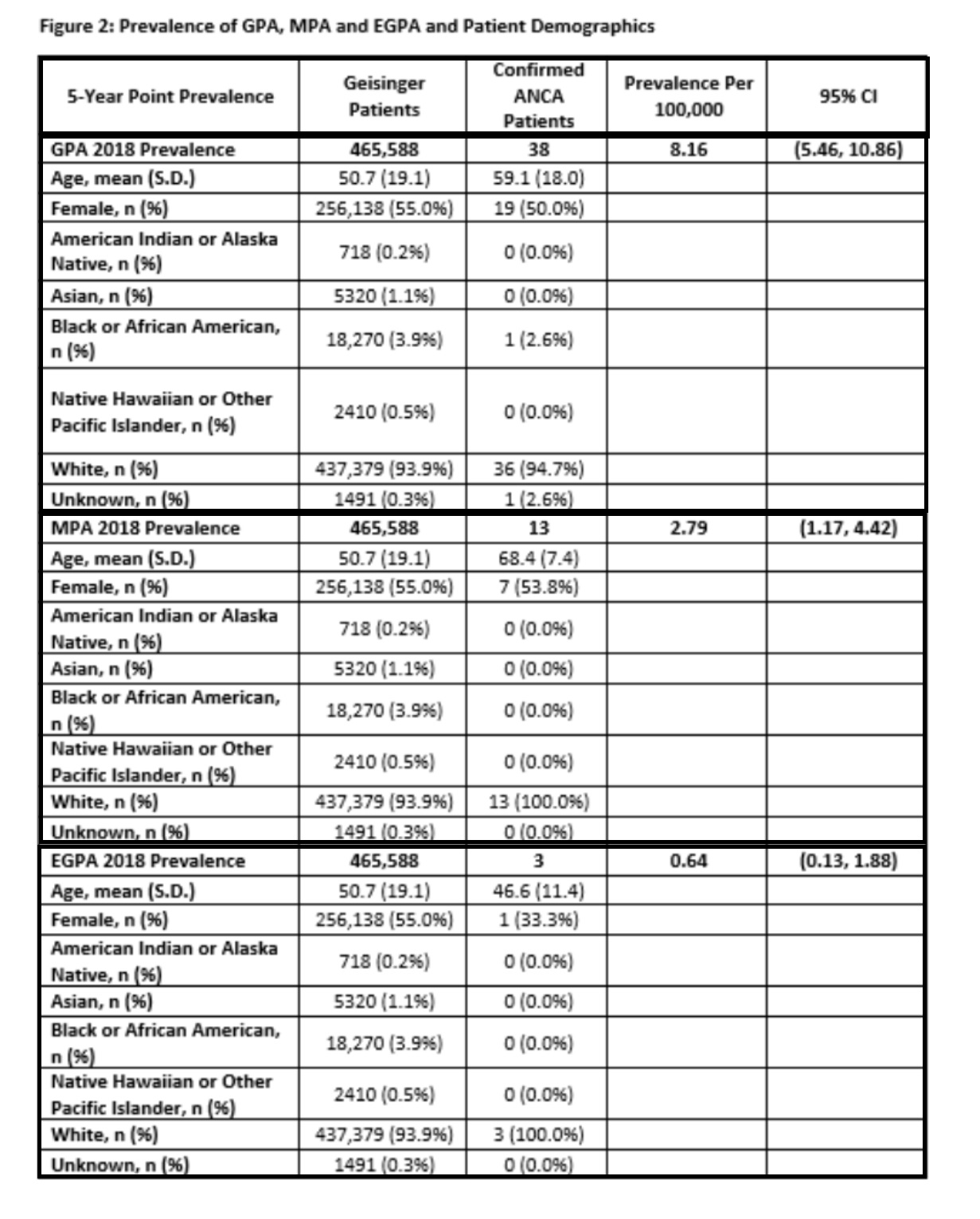
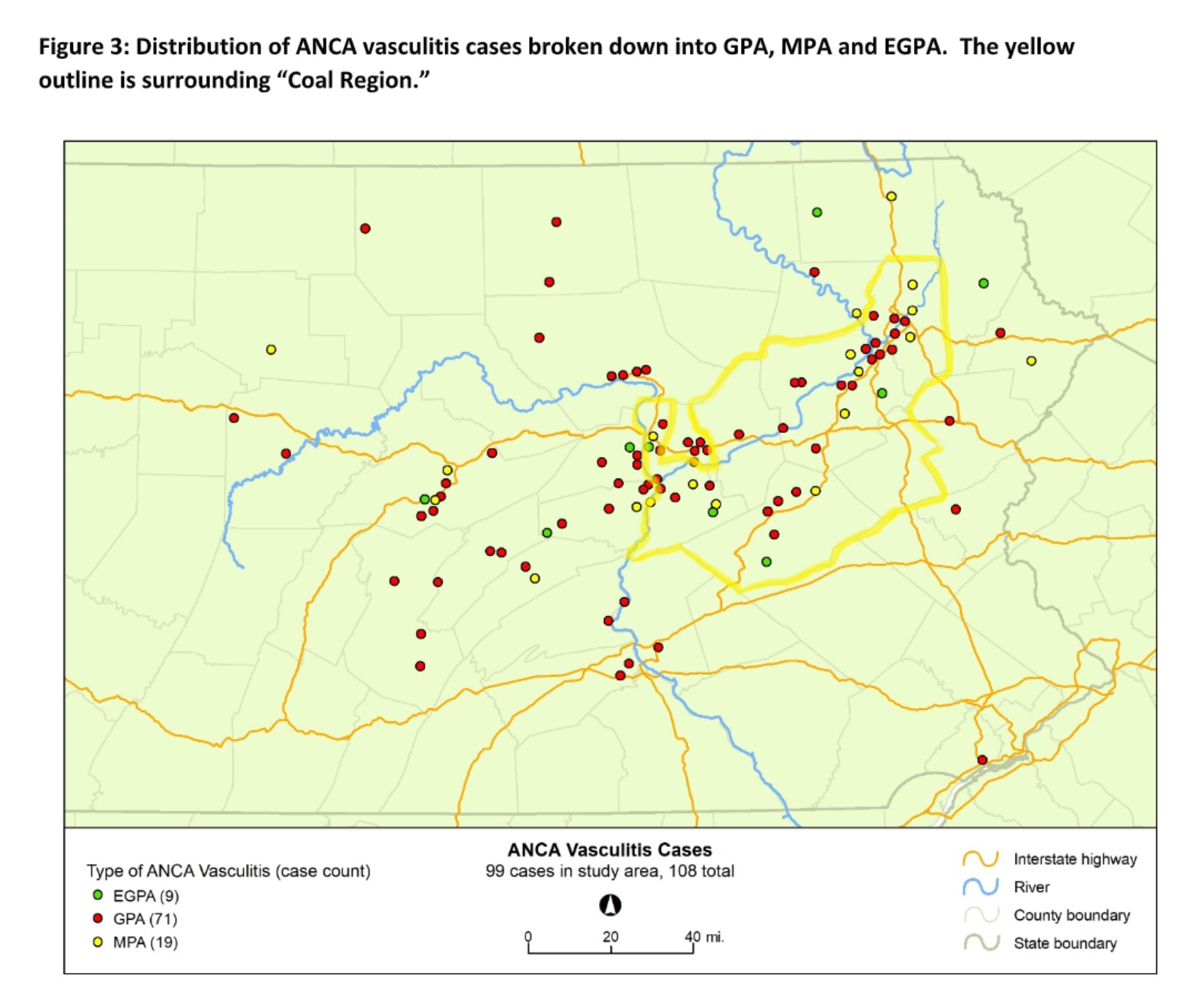
Results: Out of 2983 cases screened by ICD codes, 108 cases satisfied DCVAS. For prevalence criteria, there were 54 confirmed cases out of a denominator population of 458,588. The prevalence estimate for AAV is 11.6/ 100,000 (95% CI: 8.4, 14.8). The total population mean age was 50.7, 55.0% were female and 93.9% were Caucasian. Among the 54 AAV patients, the mean age was 60.8, 50.0% were female, and 96.3% were Caucasian. There were 38 patients with GPA, 13 with MPA, and 3 with EGPA. Prevalence estimates and demographic characteristics are shown in Figure 1 and Figure 2. The prevalence estimates for AAV and GPA is observed to be above the reported national average range. Our geographic mapping shows correlation of cases in counties deemed as Coal Region, following along a major interstate, a regional river, and primary medical service area (Figure 3).
Conclusion: Our prevalence estimates for AAV and GPA is observed to be higher than average, but MPA and EGPA has insufficient U.S. epidemiology to compare. Our health system captures a large region of predominantly Caucasian patients in a rural population so it is of interest to compare to national averages. Mapping suggests a correlation of AAV cases in Coal Region counties and along a major river, suggesting a possible environmental factor. We hope to explore potential environmental-gene interactions and compare epidemiology with an urban system in the future
To cite this abstract in AMA style:
Rottmann E, Bankert J, Berger A, Kirchner L, Dewalle J, Meissner M, George J, Bucaloiu I, Sugunaraj J, Penupolu S, Bulbin D. Epidemiology and Geographic Evaluation of ANCA-associated Vasculitis (AAV) at a Rural Academic Health Center Utilizing an Electronic Health Record (EHR) [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/epidemiology-and-geographic-evaluation-of-anca-associated-vasculitis-aav-at-a-rural-academic-health-center-utilizing-an-electronic-health-record-ehr/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/epidemiology-and-geographic-evaluation-of-anca-associated-vasculitis-aav-at-a-rural-academic-health-center-utilizing-an-electronic-health-record-ehr/