Session Information
Date: Sunday, November 7, 2021
Title: Epidemiology & Public Health Poster II: Inflammatory Arthritis – RA, SpA, & Gout (0560–0593)
Session Type: Poster Session B
Session Time: 8:30AM-10:30AM
Background/Purpose: Interstitial lung disease (ILD) is an extraarticular manifestation of RA that leads to increased morbidity and mortality. Algorithms incorporating multiple diagnostic and procedure codes as well as treating provider specialty have been developed to identify RA-ILD patients in administrative data sources. Positive predictive values (PPV) for such algorithms range between 70-85%. In this study, we adapted these RA-ILD algorithms to electronic health record (EHR) data and used text mining to capture ILD terms within chest CT reports.
Methods: We identified possible RA-ILD cases at a large academic medical center by searching the EHR for patients with at least one ICD-9/10 or SNOMED Clinical Terms code for both RA and ILD. Detailed medical record review was performed to validate RA-ILD diagnoses (reference standard). When available, chest CT images were separately reviewed by an expert in ILD for the presence/absence of ILD, blinded to the clinical data. We applied previously validated RA-ILD administrative algorithms with various combinations of ICD-9/10 codes for ILD, CPT codes for chest CT or lung biopsy, and provider specialty (pulmonology or rheumatology). Subsequently, we used text mining by automated regular expressions to identify ILD related terms (e.g. ground glass, honeycombing) and variations of these terms in chest CT reports within the EHR. We tested the performance of the aforementioned algorithms with/without these ILD terms.
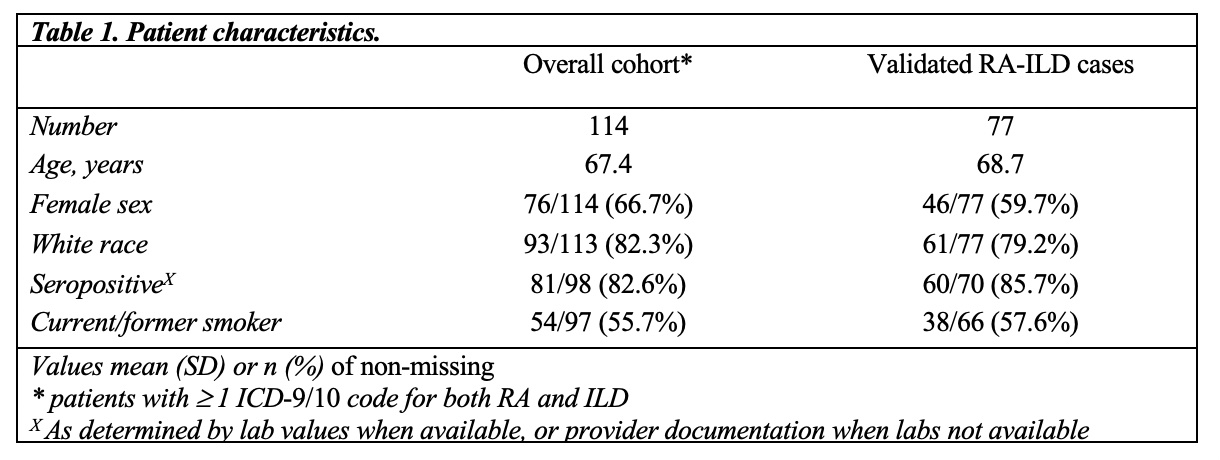
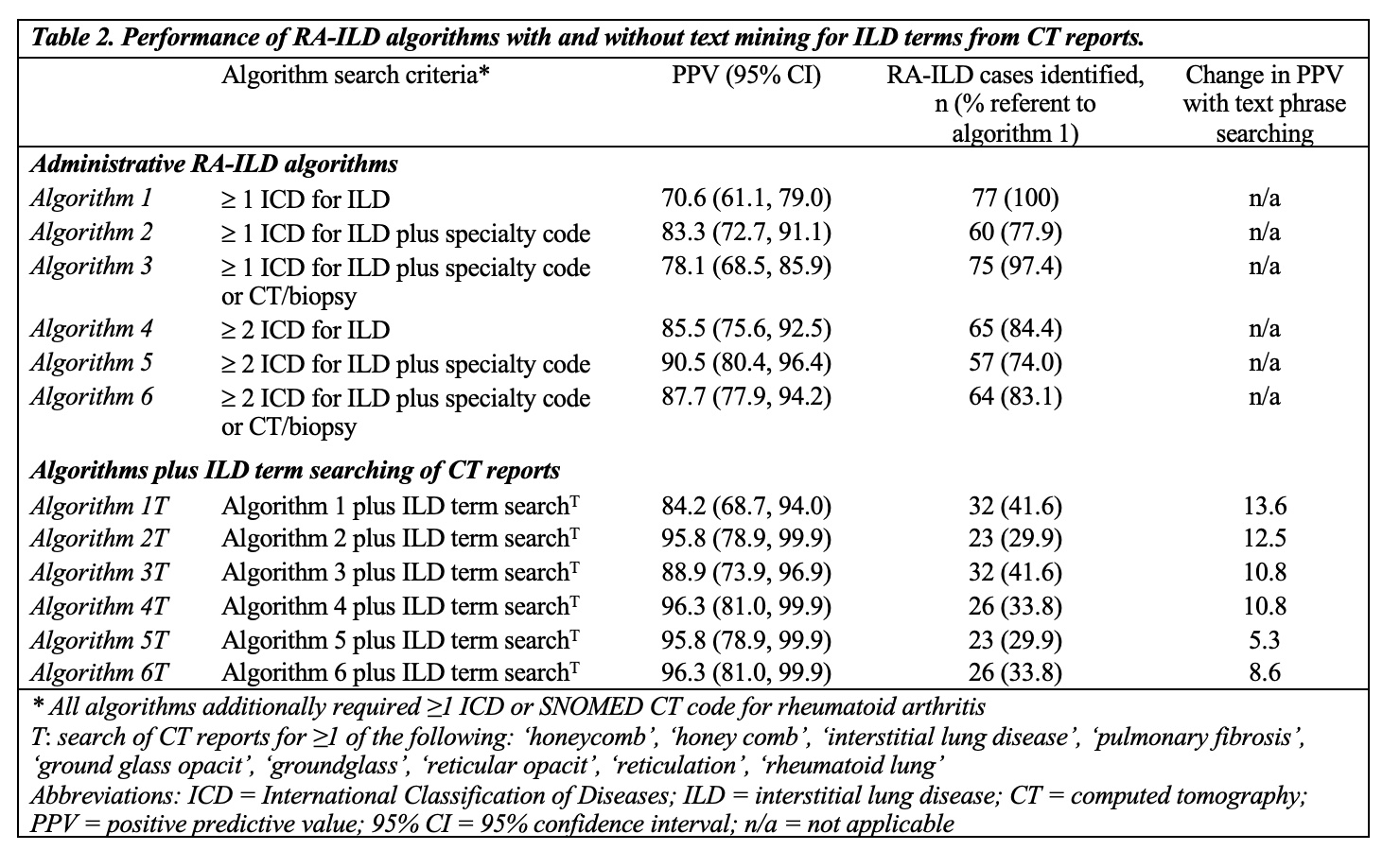
Results: Of the 114 possible RA-ILD cases, 77 were validated by record review (Table 1). Patients were on average 67.4 years old and most commonly white (82.3%), female (66.7%), and seropositive (82.6%). Among the validated RA-ILD cases, 56 had CT images available with 50 expertly read as RA-ILD (5 indeterminate). Administrative algorithms (Algorithms 1-6) had positive predictive values (PPVs) for RA-ILD ranging from 70.6 to 90.5% (Table 2). Algorithm 5 (≥2 ICD for ILD plus specialty code) had the highest PPV, but identified fewer RA-ILD cases (57/77). The addition of ILD terms extracted through text mining increased the PPV compared to similar administrative algorithms by 5-13%. Notably, adding an ILD term from chest CT to the simplest administrative algorithm (Algorithm 1T) yielded a PPV similar to the most complex administrative algorithms (Algorithms 5 and 6). Fewer RA-ILD cases were identified with ILD term searching (range 23 to 32), since many patients did not have available CT reports. Findings were similar in sensitivity analyses that considered expert read of available CTs the reference standard.
Conclusion: An ILD algorithm initially derived and validated in administrative claims data had similarly high validity when applied to EHR data. Incorporating ILD related terms from chest CT reports substantially increased the PPV, but reduced sensitivity. Declines in sensitivity due to the unavailability of CT reports may be attenuated in integrated health care systems and as data sharing across EHRs improves. Our findings demonstrate how existing administrative algorithms can be improved to better identify RA-ILD for comparative effectiveness and outcomes research that utilizes EHRs.
To cite this abstract in AMA style:
Luedders B, Cope B, Devries M, Campbell W, Campbell J, Mikuls T, Curtis J, Hershberger D, England B. Enhancing the Identification of Rheumatoid Arthritis-Associated Interstitial Lung Disease in Electronic Health Records Through Text Mining of Computerized Tomography Reports [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/enhancing-the-identification-of-rheumatoid-arthritis-associated-interstitial-lung-disease-in-electronic-health-records-through-text-mining-of-computerized-tomography-reports/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/enhancing-the-identification-of-rheumatoid-arthritis-associated-interstitial-lung-disease-in-electronic-health-records-through-text-mining-of-computerized-tomography-reports/