Session Information
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Synovial inflammation in knees with OA can be measured with musculoskeletal ultrasound (MSK US), is associated with increased pain and disease progression, and may adversely affect joint biomechanics. Knee effusion has been associated with quadriceps avoidance gait (decreased external knee flexion moment (KFM) during walking, altered quadriceps and hamstring activation) in patients with knee OA, however, the effect of treating knee inflammation on gait biomechanics and strength is unknown. The purposes of this study were to: 1) investigate the effects of treating knee inflammation on gait biomechanics, strength and patient-reported outcomes in patients with knee OA and inflammation, and 2) explore the associations between these measures.
Methods: 72 knees from 51 patients with knee OA and signs of moderate synovitis and effusion on MSK US underwent bilateral gait biomechanics, strength and US assessments, and completed knee-specific numeric rating scales (NRS) for pain and Knee Injury and Osteoarthritis Outcome Scores (KOOS) before and 3 weeks after receiving an US-guided knee aspiration and injection of 40 mg triamcinolone acetonide. Three-dimensional quantitative gait analysis was completed using a 12-camera motion capture system and floor-mounted force plate to calculate knee angles and moments, with the peak external KFM as the primary outcome. Knee extension and flexion strength (peak torque in Nm) was tested using an isokinetic dynamometer (90o/s). US assessments were performed using a linear 3-12 MHz probe. The suprapatellar recess was scanned in the long axis view (medial, lateral, midline) with the knee flexed to 20o. All US exams were graded using the OMERACT system for inflammatory features of knee OA. Paired T-tests were used to determine mean changes and 95% confidence intervals from pre to 3 weeks post injection for all measures. Mixed effects regression with robust sandwich estimators was then used to evaluate the associations between potential predictors and peak KFM during walking. Random intercepts and slopes were specified by patient ID, time and limb. Potential predictors included US regional score (0-9), effusion depth (mm), gait speed (m/s), NRS (0-10), and quadriceps strength (Nm). Only knees undergoing aspiration and injection were evaluated.
Results: Baseline demographic and clinical characteristics are presented in Table 1. US regional score, effusion depth and NRS pain decreased post injection (Table 2). The peak KFM during walking, quadriceps and hamstring strength and KOOS subscales (symptoms, pain, daily living) increased post injection (Table 2). While controlling for time and limb, increases in gait speed and reductions in NRS pain were associated with greater peak KFM (Table 3).
Conclusion: Aspiration and corticosteroid injection improves signs of inflammation on MSK US, gait biomechanics associated with quadriceps avoidance gait, strength, and patient-reported measures of pain and function in patients with knee OA. Greater gait speed and lesser knee pain were associated with less quadriceps avoidance gait. This suggests that local knee inflammation may contribute to abnormal gait biomechanics, however, further research is needed to understand the mechanism.
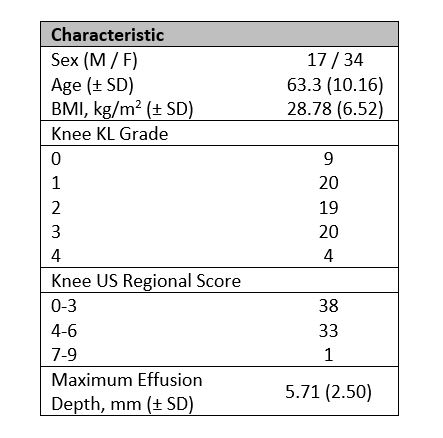 Table 1. Demographic and clinical characteristics (n=51 patients, 72 knees)
Table 1. Demographic and clinical characteristics (n=51 patients, 72 knees)
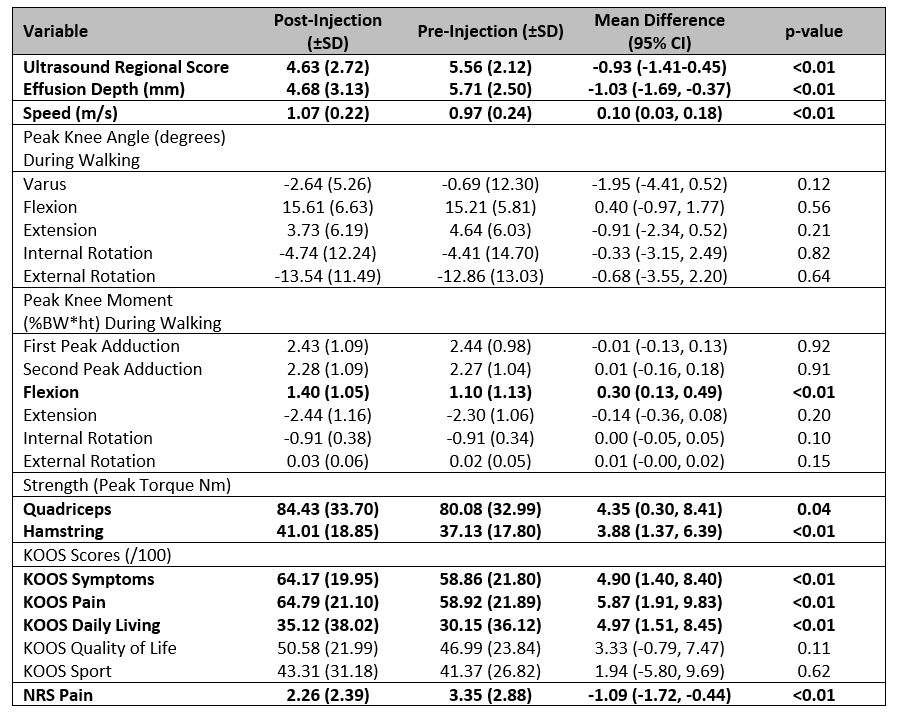 Table 2. Descriptive statistics for outcome measures pre and 3 weeks post injection.
Table 2. Descriptive statistics for outcome measures pre and 3 weeks post injection.
 Table 3. Linear mixed effects model estimates
Table 3. Linear mixed effects model estimates
To cite this abstract in AMA style:
Pinto R, Birmingham T, Philpott H, Arsenault D, Primeau C, Appleton T. Effect of Knee Aspiration and Intra-articular Corticosteroid Injection on Gait Biomechanics and Strength Impairment in Patients with Signs of Inflammation Due to Knee Osteoarthritis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/effect-of-knee-aspiration-and-intra-articular-corticosteroid-injection-on-gait-biomechanics-and-strength-impairment-in-patients-with-signs-of-inflammation-due-to-knee-osteoarthritis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/effect-of-knee-aspiration-and-intra-articular-corticosteroid-injection-on-gait-biomechanics-and-strength-impairment-in-patients-with-signs-of-inflammation-due-to-knee-osteoarthritis/