Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Systemic Juvenile Idiopathic Arthritis (sJIA) is a systemic autoinflammatory disease characterized by high fevers, rash and arthritis. Current treatment regimens often involve biologic (anti-IL-1 or anti-IL6) medications, glucocorticoids (GC), or both. Both treatments and disease can have a significant impact on health-related quality of life (HRQoL). GC may be used in addition to biologic treatment for many reasons, including concern that the biologic medication alone may not be enough to control severe systemic disease or pain. This study aimed to evaluate the impact of early use of GC on HRQoL in newly diagnosed sJIA patients started on a biologic treatment.
Methods: Data on patient reported outcomes (PROs) was collected as part of the FiRst-line Options for Systemic juvenile idiopathic arthritis Treatment (FROST) study, a non-randomized prospective observational study of outcomes in children with newly diagnosed sJIA treated by one of 4 Childhood Arthritis and Rheumatology Research Alliance (CARRA) consensus treatment plans (CTPs) for sJIA enrolled in the CARRA Registry. Treatment, including GC use, was at the discretion of the treating provider. This analysis included only subjects treated with a biologic (anti-IL1 or anti-IL6) CTP. Early GC usage was defined as any use reported at the baseline, 2 week, or 1 month visit. Patients were evaluated by their treating physician at baseline, week 2, and months 1, 3, 6, 9, and 12; PROs collected at these visits included patient global disease assessment and Patient Reported Outcomes Measurement Information Systems (PROMIS) short forms. Home PROs on pain, fever, and rash were collected every 2 days for 4 weeks, then weekly for 3 months. Generalized estimating equations and linear mixed effects models were used to compare PROs between GC treatment groups.
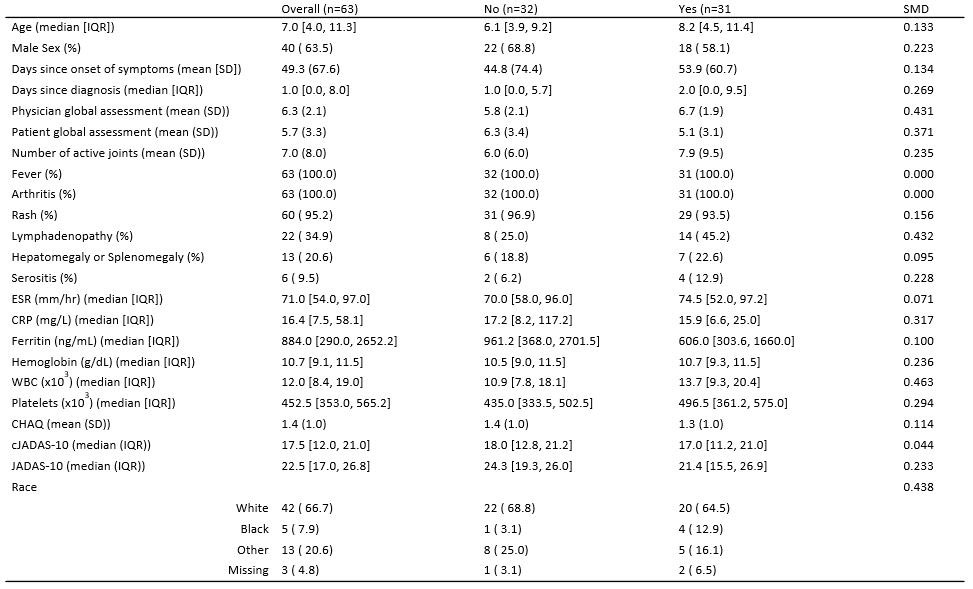
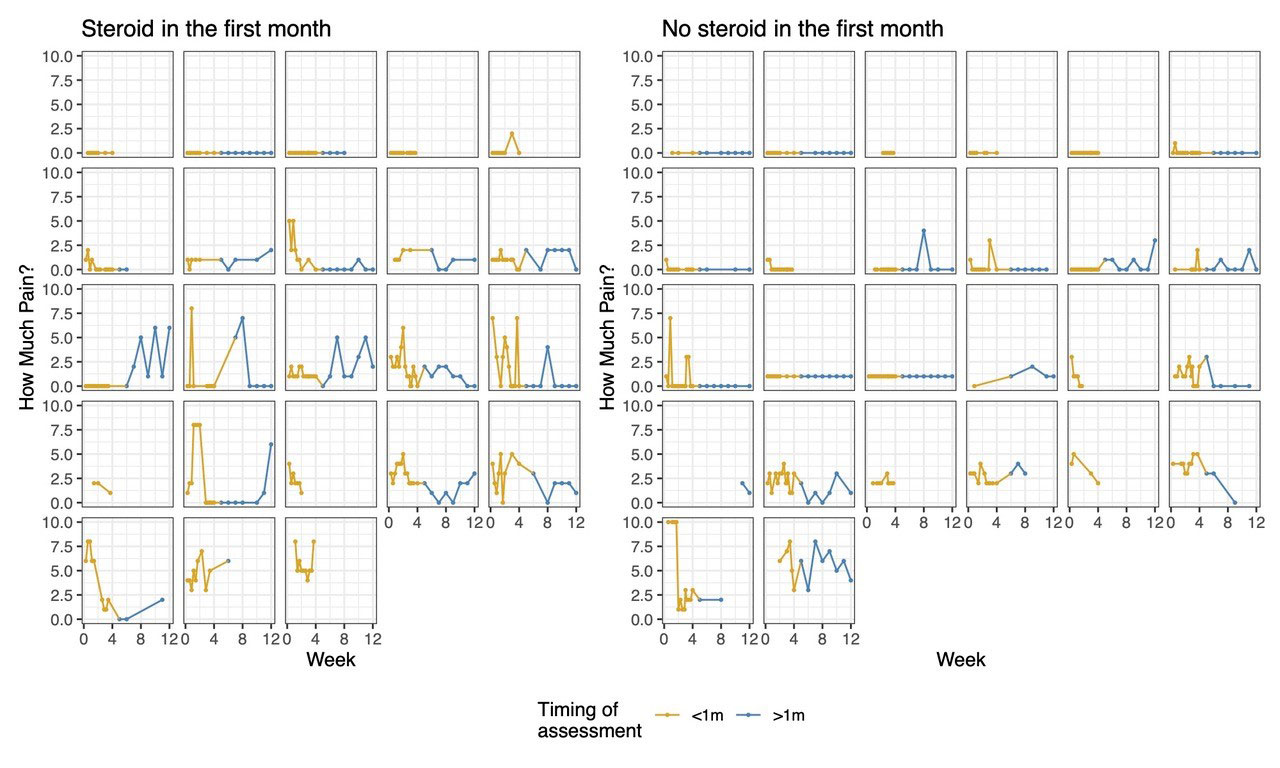
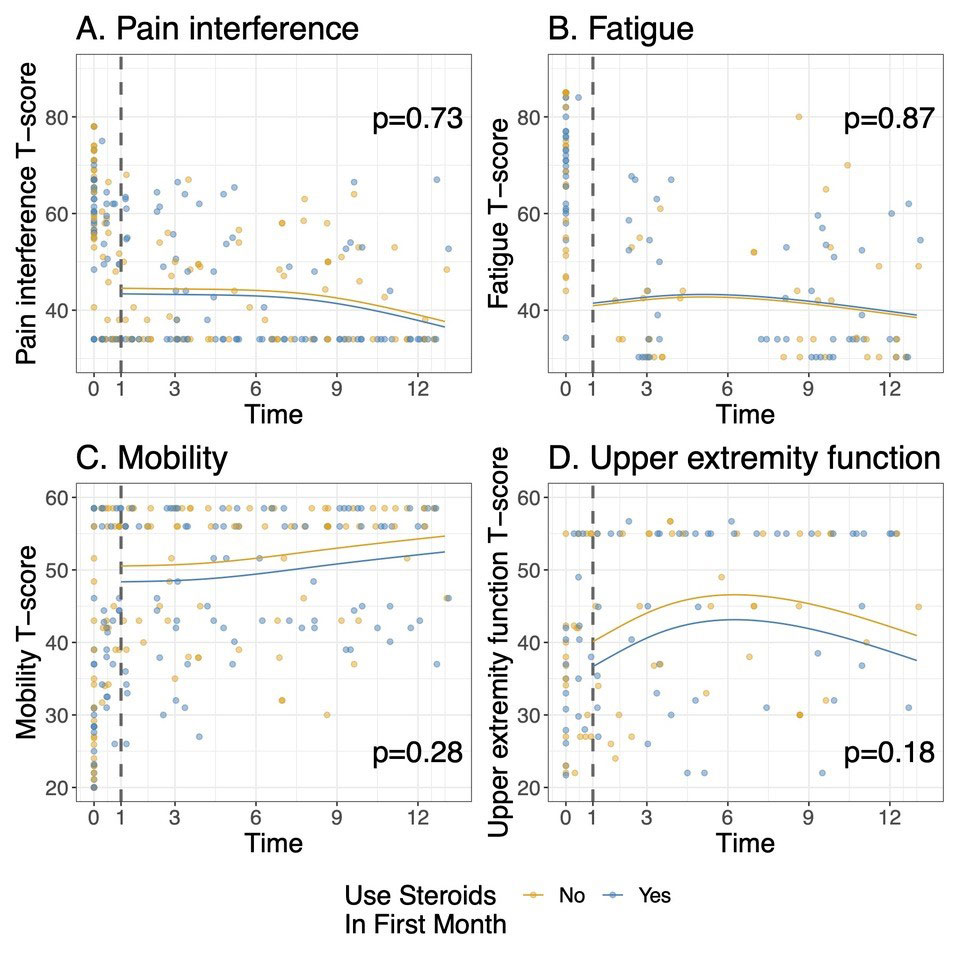
Results: 63 of the 73 subjects enrolled in FROST began one of the biologic CTPs. The median age was 7 years (IQR 4.0, 11.3), and 64% were male. 31 (49%) received GC within the first month. Baseline disease characteristics of subjects by GC treatment group are shown in table 1. Subjects treated with GC had a higher median baseline joint count and physician global assessment of disease activity, but a lower CRP and patient global assessment of disease activity. (Table 1). No significant differences were noted in patient reported pain from home over the first 12 weeks in those receiving GC in the first month vs those not (p=0.71, Figure 1), or over the first year of follow-up in terms of PROMIS scores on pain interference (p=0.73), fatigue (p=0.87), mobility(p=0.28), or upper extremity function (p=0.18), after adjusting for time and baseline joint count. (figure 2)
Conclusion: Although GC’s were given at the providers’ discretion, patients had very similar baseline characteristics regardless of GC treatment group. There were no significant differences in the trend of improvement in most PROs over the first year of treatment, with point estimates for mobility, pain interference, and upper extremity function appearing better in the group not treated with GC, even after adjusting for joint count. This suggests that early GC use, when used with biologics, may not have significant effects in the patient’s experience of their disease.
K. James, None; G. Tomlinson, None; T. Beukelman, Novartis, UCB; L. Schanberg, UCB, Sanofi; A. Dennos, None; V. Del Gaizo, None; M. Jelinek, None; E. Pfeifer, genentech; S. Mohan, genentech; Y. Kimura, Genentech.
To cite this abstract in AMA style:
James K, Tomlinson G, Beukelman T, Schanberg L, Dennos A, Del Gaizo V, Jelinek M, Pfeifer E, Mohan S, Kimura Y. Effect of Glucocorticoids on Patient Reported Outcomes in Patients Started on a Biologic Consensus Treatment Plan for the ‘First Line Options for Systemic JIA Treatment’ (FROST) Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/effect-of-glucocorticoids-on-patient-reported-outcomes-in-patients-started-on-a-biologic-consensus-treatment-plan-for-the/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/effect-of-glucocorticoids-on-patient-reported-outcomes-in-patients-started-on-a-biologic-consensus-treatment-plan-for-the/