Session Information
Session Type: Abstract Session
Session Time: 4:00PM-4:15PM
Background/Purpose: Bone marrow lesions (BMLs) and effusion-synovitis are frequent and dynamic disease processes detected from early- to late-stage knee OA. These processes are associated with knee symptoms, representing the primary clinical manifestations of OA. Through a systematic and iterative process, we previously developed and validated a composite biomarker – the disease activity metric – that combines BML and effusion-synovitis volumes throughout a knee into an efficient continuous single score. It remains unclear whether this composite score represents clinically meaningful pathways to early stages of OA and if it could detect people early, before the onset of OA. We evaluated whether these dynamic disease processes (effusion-synovitis volume and BMLs), summarized by a validated efficient continuous composite score, are present in early OA and prognostic of incident symptomatic knee OA over the subsequent three years.
Methods: We analyzed a convenience sample within the Osteoarthritis Initiative (OAI) of participants without symptomatic knee OA. Pain assessments and radiographs were collected annually. Using magnetic resonance images from the initial visit, we combined effusion-synovitis and BML volumes (intra-reader ICCs ≥ 0.95) to calculate a composite score, referred to as the disease activity metric. A disease activity metric of 0 corresponded to the average in a reference sample (n=197, 53% with moderate-severe radiographic knee OA, average [SD] WOMAC pain score = 5.0 [3.6]); lower (negative) values indicate milder disease, while greater values indicate worse disease. The outcome was incident symptomatic knee OA (the combined state of frequent knee pain and radiographic OA [Kellgren-Lawrence Grade ≥ 2]) within three years after the disease activity measurement. We used logistic regression with repeated measures to examine the association between disease activity (continuous and tertiles) and incident symptomatic knee OA, adjusting for gender, age, and body mass index.
Results: Among 913 knees (n=572 participants), most were female (56%), white (82%), and had a mean age of 61 (SD=9) and body mass index of 29.4 (SD=4.5) kg/m2. Disease activity ranged from -3.8 to 24.8 (lower values = smaller effusion-synovitis and BML volumes). Knees that developed incident symptomatic OA had a greater mean disease activity metric compared to those that did not (-0.3 [2.7] vs. -1.4 [2.7]). The adjusted relative risk of incident symptomatic OA per 1 unit increase in disease activity was 1.08 (95% confidence interval: 1.04-1.11). Stratified analyses suggested that the association was driven by knees with either radiographic OA only or symptoms only at baseline.
Conclusion: Our findings underscore the critical role of the composite disease activity metric in the early detection of knee OA. By integrating BMLs and effusion-synovitis volumes, this metric provides a powerful prognostic tool, enabling earlier detection and potential intervention to alter disease progression. These results also support the development of targeted therapies that address inflammation and bone turnover in early OA.
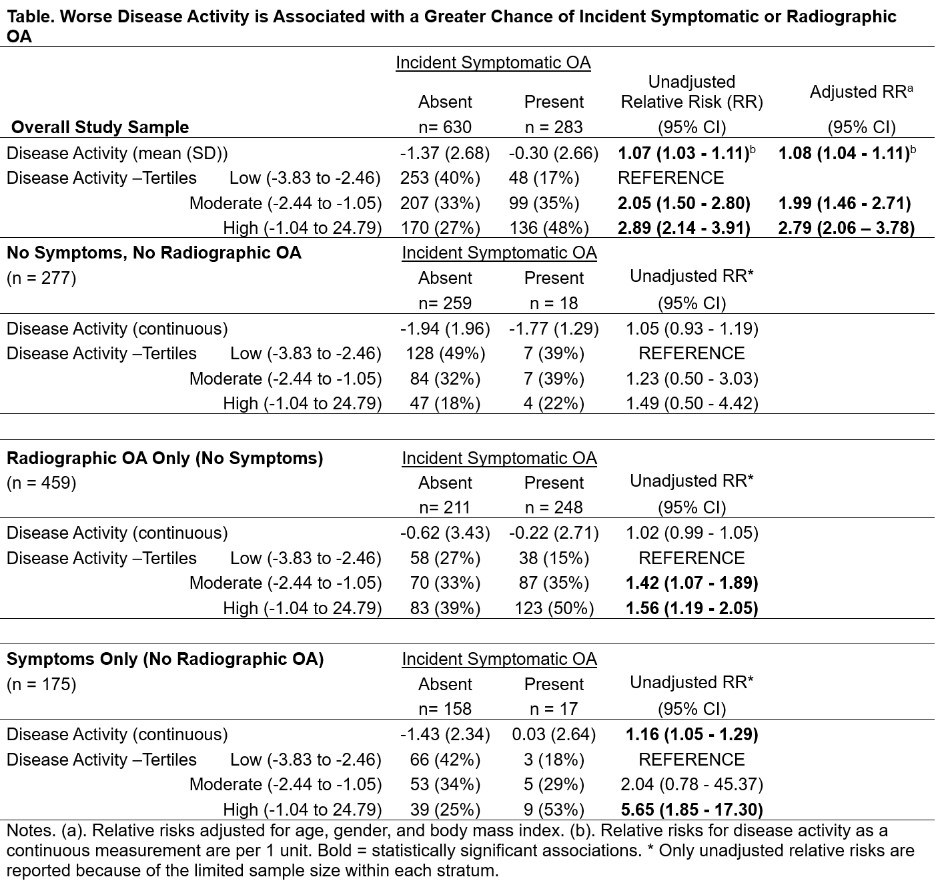 Table. Worse Disease Activity is Associated with a Greater Chance of Incident Symptomatic or Radiographic OA
Table. Worse Disease Activity is Associated with a Greater Chance of Incident Symptomatic or Radiographic OA
Disclosures: J. Patarini: None; T. McAlindon: Anika, 2, Grunenthal, 2, Kiniksk, 2, Kolon TissueGene, Inc., 2, Medipost, 2, Novan, 2, Organogenesis, 2, Regeneron, 2, Remedium-Bio, 2, Samumed, 2, Sanofi, 2, Scarcell, 2, Visor, 2; J. Baek: None; E. Kirillov: None; N. Vo: None; M. Richard: None; M. Zhang: None; M. Harkey: None; G. Lo: None; S. Liu: None; K. Lapane: None; C. Eaton: None; J. Mackay: AstraZeneca, 3, Blue Earth Diagnostics, 3; J. Driban: None.
To cite this abstract in AMA style:
Patarini J, McAlindon T, Baek J, Kirillov E, Vo N, Richard M, Zhang M, Harkey M, Lo G, Liu S, Lapane K, Eaton C, Mackay J, Driban J. Early Detection of Knee Osteoarthritis – The Role of a Composite Disease Activity Metric: Data from the Osteoarthritis Initiative [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/early-detection-of-knee-osteoarthritis-the-role-of-a-composite-disease-activity-metric-data-from-the-osteoarthritis-initiative/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/early-detection-of-knee-osteoarthritis-the-role-of-a-composite-disease-activity-metric-data-from-the-osteoarthritis-initiative/