Session Information
Date: Sunday, November 5, 2017
Title: Osteoarthritis – Clinical Aspects I: Pain and Functional Outcomes
Session Type: ACR Concurrent Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Therapeutic exercise is the recommended non-pharmacological treatment for knee osteoarthritis (OA). However, the optimal treatment dose and clinically meaningful treatment durations remain unclear. Our purpose was to examine dose-response relationships, the minimum effective dose, and baseline factors associated with the timing of response from two exercise interventions among adults with symptomatic knee OA.
Methods: Secondary analysis of a single-blind, randomized trial comparing 12-week Tai Chi and Physical Therapy exercise programs among adults with symptomatic knee OA (ACR Criteria). WOMAC pain (0-500) and function (0-1700) scores were completed each week of intervention. We defined dose as attendance-weeks (i.e. total treatment weeks attended), and treatment response as ≥20% and ≥50% improvement in pain and function. Using log-rank tests, we compared time-to-response between interventions, and used Cox regression to examine baseline factors associated with the timing of response (≥50% improvement only).
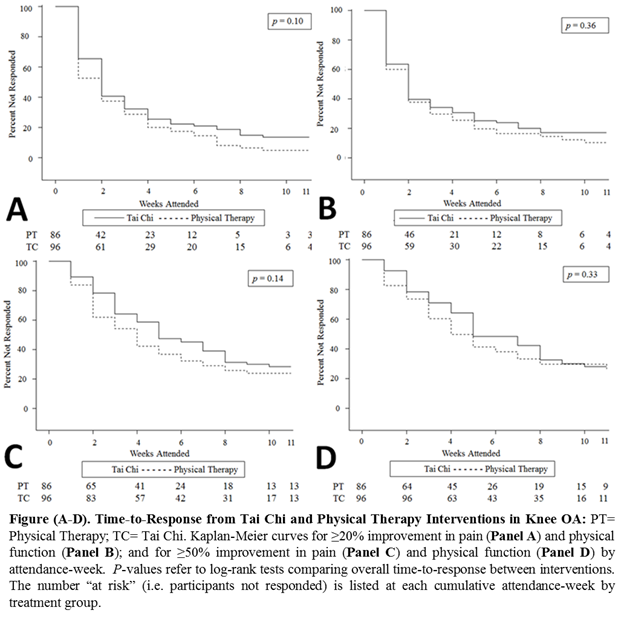
Results: We examined 182 participants (mean age 61 years, BMI 32 kg/m2, 70% female, 55% white). Both interventions had linear dose-response effect resulting in a 9 to 11-point reduction in WOMAC pain and a 32 to 41-point improvement in function per week. There was no significant difference in overall time-to-response for pain and function between treatment groups (Figure). Median time-to-response for ≥20% improvement in pain and function was 2 attendance-weeks and 4 to 5 attendance-weeks for ≥50% improvement. On unadjusted models, we found a general pattern wherein physical health factors, self-efficacy, and outcome expectations tended to be significantly associated with treatment response rather than psychosocial or biomechanical factors (Table). On multivariable models, outcome expectations were independently associated with incident function response (Hazard Ratio: 1.47; 95% CI: 1.004 to 2.14).
Conclusion: Both interventions had linear dose-dependent effects on pain and function, their minimum effective doses ranged from 2 (≥20% improvement) to 5 weeks (≥50% improvement), and patient-perceived benefits of exercise independently influenced the timing of response among adults with symptomatic knee OA. These results may help clinicians optimize patient-centered exercise treatments and better manage patient expectations.
|
Table. Unadjusted Hazard Ratios of Treatment Response (≥50% improvement) in Pain and Physical Function by Baseline Factors (n=182) |
|||
|
Characteristic |
Hazard Ratio (95% Confidence Interval) |
||
|
|
Pain |
Function |
|
|
Age, years |
1.01 (0.99, 1.03) |
1.02 (1.00, 1.04) |
|
|
Female Sex, n (%) |
1.32 (0.87, 2.01) |
1.29 (0.85, 1.96) |
|
|
Race, n (%) |
|
|
|
|
White |
reference |
reference |
|
|
Black |
0.71 (0.47, 1.07) |
0.59 (0.39, 0.91) |
|
|
Asian/Other |
0.94 (0.53, 1.67) |
0.91 (0.52, 1.58) |
|
|
Body Mass Index, kg/m2 |
0.98 (0.96, 1.01) |
0.98 (0.95, 1.00) |
|
|
Duration of knee pain, years |
1.01 (1.00, 1.03) |
1.01 (1.00, 1.03) |
|
|
Highest Level of Education, n (%) |
|
|
|
|
High school graduate or less |
reference |
reference |
|
|
Some college or more |
1.69 (0.97, 2.94) |
1.85 (1.02, 3.36) |
|
|
WOMAC Pain (Range: 0-500); (50-point units) |
n/a |
0.86 (0.78, 0.95) |
|
|
WOMAC Physical Function (Range: 0-1700); (100-point units) |
0.96 (0.91, 1.004) |
n/a |
|
|
Patient Global Assessment (Range: 0-10cm) |
0.87 (0.80, 0.94) |
0.88 (0.81, 0.96) |
|
|
SF-36 Physical Component Summary (Range: 0-100)#; (10-point units) |
1.35 (1.10, 1.65) |
1.46 (1.18, 1.81) |
|
|
PROMIS Sleep disturbance (Range, T-Score: 28.9-76.5); (10-point units) |
0.88 (0.74, 1.05) |
0.83 (0.69, 1.00) |
|
|
SF-36 Energy and Vitality (Range: 0-100)#; (10-point units) |
1.06 (0.96, 1.17) |
1.08 (0.97, 1.19) |
|
|
CHAMPS Physical Activity moderate-high calories/week# (500-calories/week units) |
1.05 (1.003, 1.10) |
1.06 (1.009, 1.11) |
|
|
6-Minute Walk Test meters# (50-meter units) |
1.12 (1.01, 1.25) |
1.14 (1.03, 1.27) |
|
|
Arthritis Self-Efficacy Scale-8 (Range: 0-10)# |
1.11 (1.01, 1.21) |
1.14 (1.04, 1.25) |
|
|
Outcome Expectations (Range: 1.0-5.0)# |
1.14 (0.82, 1.57) |
1.43 (1.03, 1.97) |
|
|
CHAMPS= Community Healthy Activities Model Program for Seniors; PROMIS= Patient-Reported Outcomes Measurement Information Systems; SF-36= Short Form-36; WOMAC= Western Ontario and McMasters Osteoarthritis Index. *Normal range reported for the general population. #Higher score indicates greater health. |
|||
To cite this abstract in AMA style:
Lee A, Harvey WF, Price LL, Han X, Driban JB, Iversen MD, Bannuru RR, Wang C. Dose-Response Effects of Tai Chi and Physical Therapy Exercise Interventions in Symptomatic Knee Osteoarthritis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/dose-response-effects-of-tai-chi-and-physical-therapy-exercise-interventions-in-symptomatic-knee-osteoarthritis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/dose-response-effects-of-tai-chi-and-physical-therapy-exercise-interventions-in-symptomatic-knee-osteoarthritis/