Session Information
Date: Monday, November 9, 2020
Title: RA – Diagnosis, Manifestations, & Outcomes Poster IV: Lifespan of a Disease
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Preventive medical care improves morbidity and mortality. The assessment included 28,105 RA patients from prospective randomized trials.
Methods: Nested data from a single site was compared to global data in 34 pivotal studies using immune therapies for RA. Another 5 studies in long term follow up in older RA patients were also analyzed. Data was extracted from NDAs submitted for FDA approval for 5 TNFi therapies, 5 JAKi therapies, rituximab, abatacept, IL-1, and IL-6 therapy. The nested site participated in each study, so entry criteria, age, concomitant medication, and intervention were identical. All subjects fulfilled the ACR criteria for RA and trials had IRB approval. Safety results for the global sites in the NDA are available to the public from accessdata.fda.gov. Safety data of special interest were incidence of death from any cause, MACE, pneumonia, and zoster. The nested site instituted 10 specific preventive care measures. These included:
1) vaccination for influenza, pneumonia, and zoster; 2) hypertensive treatment for blood pressure >140/90; 3) diabetes treatment if HbA1C >9; 4) treatment for uric acid >7; 5) statin therapy if LDL >120; 6) treatment if BMI >30 including staff dietician every 3 months; 7) chewable aspirin 81 mg/d; 8) prenatal vitamin for 1 mg folate; 9) daily sinus wash to decrease URI (NeilMed); 10) no use of corticosteroids or narcotics. All preventive measures were conducted at the nested site.
Results: (tables 1, 2, 3)
Zoster: There were 18,696 subjects in JAKi trials in the global population and 562 at the nested site. Zoster incidence in trials using JAKi decreased between 2005-2020. Key to this decline was Zostavax approval in 2006 and Shringrix approval in 2017. At the nested site, zoster vaccines for all started in 2006.
Pneumonia and Death due to Infection: There were 28,105 subjects in the global population and 924 subjects at the nested site. Pneumonia events were lower in the nested site than the global population, both in the long term trials (ages 63-70) and in the shorter trials (ages 51-53). All nested site subjects had pneumonia vaccination. Deaths due to infection were lower at the nested site (about one third of deaths in RA were due to pneumonia).
Mortality: There were 4469 global subjects and 154 at the nested site in the older population of the long term trials. Mortality was less at the nested site in these older subjects. In the shorter trials with younger subjects, of the 28,105 global subjects and 924 in the nested site, overall mortality was not different.
Mace: MACE events were not better at the nested site for the older population (followed 3-7 years) nor the younger population (followed 6 months to 2 years).
Thrombotic events
The nested site had fewer thrombotic events in the JAKi trials and subjects took chewable aspirin 81 mg/d.
Conclusion: This is a causal inference study using prospective data from 39 trials. Vaccination is a likely explanation for less zoster, pneumonia, infectious deaths, and mortality at the nested site. The lack of any data over 10 years limits efforts to measure reduction of uncommon MACE events (control of blood pressure, diabetes, cholesterol and diet). Vaccines are clearly necessary in medical care for RA. Vetted data from NDAs can yield insight for healthcare.
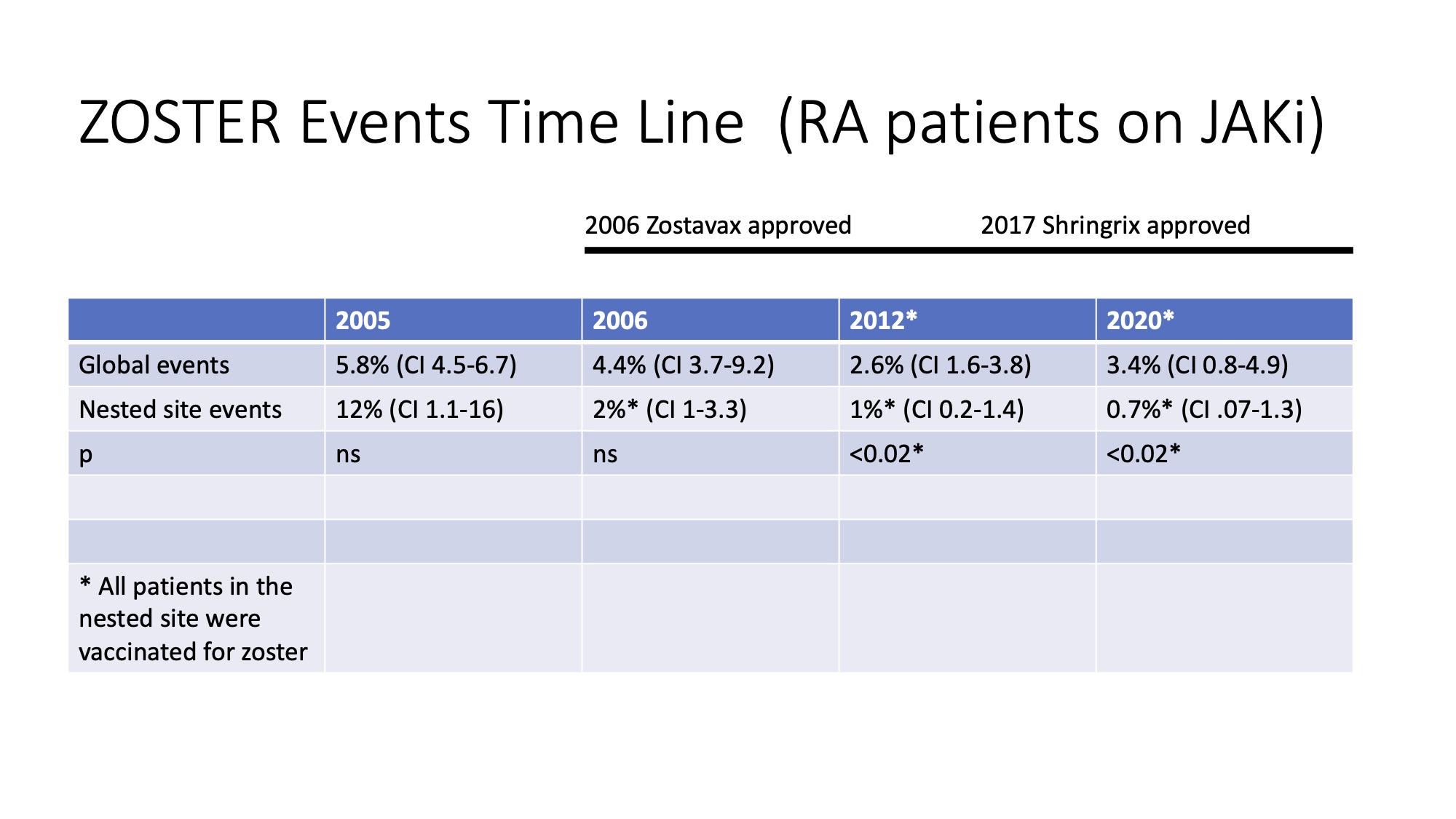 Table 1
Table 1
 Table 2
Table 2
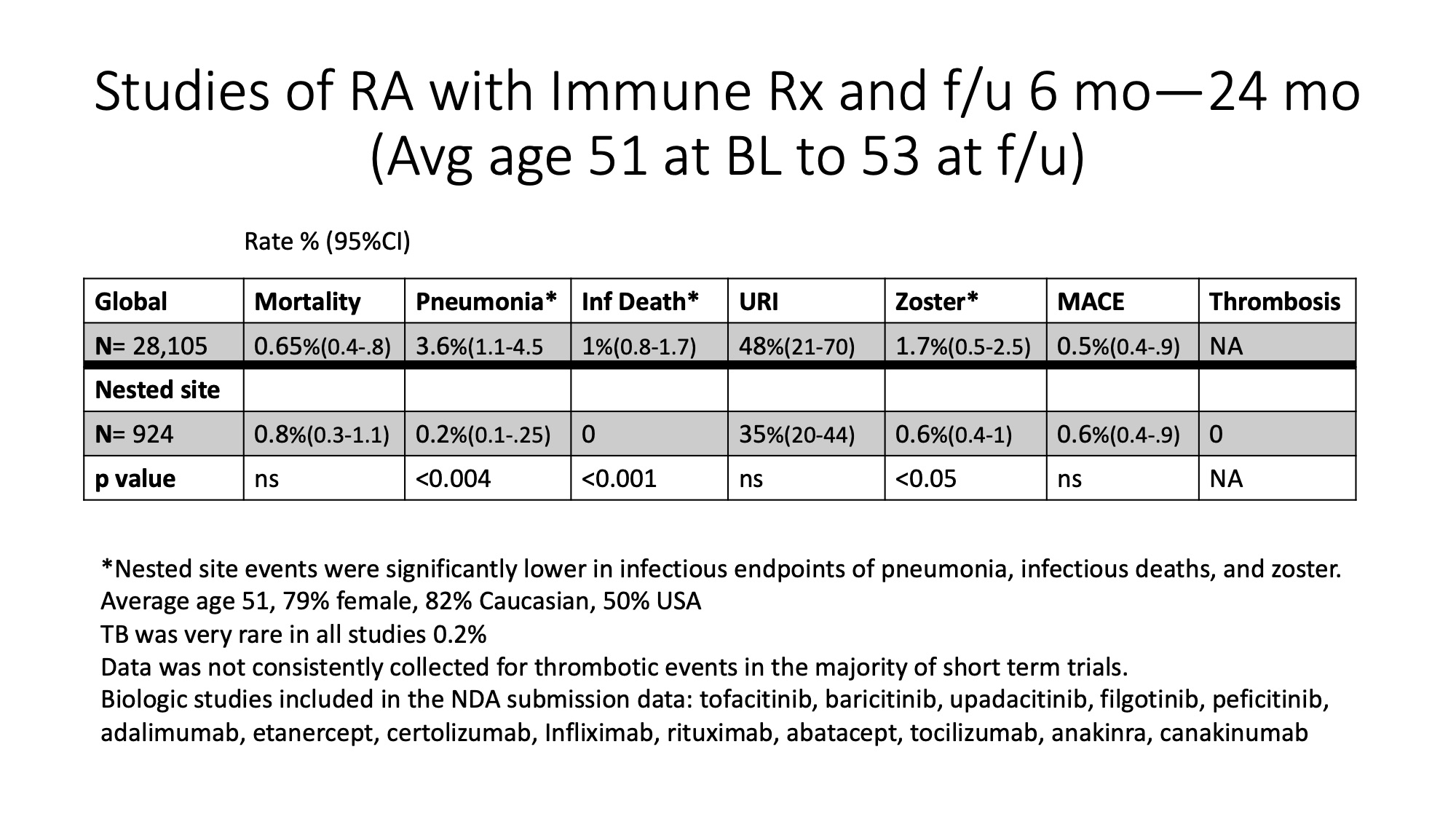 Table 3
Table 3
To cite this abstract in AMA style:
Greenwald M, Ball J, Lopez S, Berg M, Greenwald M. Does Preventive Care Matter? (in RA) [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/does-preventive-care-matter-in-ra/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/does-preventive-care-matter-in-ra/