Session Information
Date: Sunday, November 5, 2017
Title: Systemic Lupus Erythematosus – Clinical Aspects and Treatment Poster I: Biomarkers and Outcomes
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Methods: Retrospective analysis of laboratory parameters, clinical activity, infection and serositis in consecutive SLE patients between 2006 and 2015. Based on the treating physician´s judgement on disease activity and presence of infection, patients were separated into four groups: flare, infection, both and neither. ESR was correlated to CRP, ferritin, anti-dsDNA antibodies, C3, serositis and erythrocyturia with proteinuria. For age, ESR, CRP, ferritin and age- and gender-adapted ESR (ESRp), mean values between groups were compared. ESRp was calculated as the percentage of an ESR cut-off considering age and gender.
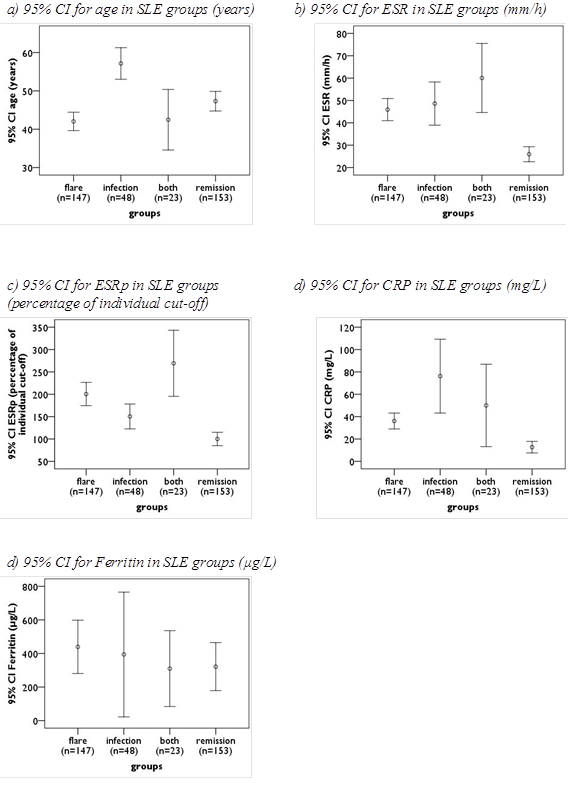
Results: We identified 203 SLE patients with 371 visits, flare n=147, infection n=48, both n=23 and neither flare nor infection n=153. Correlation coefficients of ESR and other parameters are given in table 1; there was moderate correlation with CRP (r=0.47-0.58) and weak correlation with other parameters (r<0.2). As shown in figure 1, ESR and CRP levels were normal in patients in remission, but did not differ between flare, infection or both. ESRp was higher in patients with flare versus with infection (p=0.01). ESR and CRP lost association to activity in infected patients and, conversely, to infection in patients with flare. ESRp, serositis and anti-dsDNA antibodies were related to disease activity regardless of infections (table 2).
Conclusion: ESR is raised in flares, but also in infected and older patients. CRP levels do not enable discrimination between flare and infection. Both parameters argue against flare and infection when normal. ESRp can help to differentiate between flare, infection or even both.
Table 1: Correlation coefficients of ESR with other laboratory and clinical parameters
|
|
CRP |
Ferritin |
C3-reduction |
Raised anti-dsDNA-antibodies |
erythrocyturia + proteinuria |
Serositis |
|
All visits (n=371) |
0.498* |
0.256* |
0.165* |
0.134* |
0.186* |
0.079 |
|
Flare only (n=147) |
0.549* |
0.268* |
0.064 |
0.101 |
0.141 |
0.094 |
|
Infection only (n=48) |
0.468* |
0.109 |
0.172 |
0.12 |
0.214 |
-0.338* |
|
Both (n=23) |
0.575* |
0.266 |
0.037 |
0.205 |
0.091 |
-0.09 |
|
Silent (n=153) |
0.556* |
0.25 |
0.032 |
0.082 |
0.137 |
-0.016 |
(Pearson´s r); significant correlation is marked with *.
Table 2: Association of laboratory and clinical parameters with SLE flare and infection
|
|
ESR |
ESRp |
CRP |
Ferritin |
C3-reduction |
Raised anti-dsDNA-antibodies |
Erythrocyturia + Proteinuria |
Serositis |
|
P-value for the association with disease activity |
||||||||
|
all visits (n=371) |
<0.001* |
<0.001* |
0.692 |
0.405 |
<0.001* |
<0.001* |
0.002* |
<0.001* |
|
without infection (n=300) |
<0.001* |
<0.001* |
<0.001* |
0.318 |
<0.001* |
<0.001* |
0.01* |
<0.001* |
|
with infection (n=71) |
0.186 |
<0.001* |
0.321 |
0.713 |
0.268 |
<0.001* |
– |
0.05* |
|
P-value for the association with infections |
||||||||
|
all visits (n=371) |
<0.001* |
0.053 |
<0.001* |
0.797 |
0.384 |
0.023* |
0.831 |
0.474 |
|
without activity (n=201) |
<0.001* |
0.001* |
<0.001* |
0.642 |
0.281 |
0.068 |
1 |
0.766 |
|
with activity (n=170) |
0.039 |
0.052 |
0.213 |
0.576 |
0.255 |
1 |
0.506 |
1 |
Figure 1: 95% confidence interval of mean values of age, ESR, ESRp, CRP, and ferritin in SLE groups
To cite this abstract in AMA style:
Schäfer VS, Weiss K, Krause A, Schmidt WA. Does Erythrocyte Sedimentation Rate Reflect and Discriminate Flare from Infection in Systemic Lupus Erythematosus? Correlation with Clinical and Laboratory Parameters of Disease Activity [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/does-erythrocyte-sedimentation-rate-reflect-and-discriminate-flare-from-infection-in-systemic-lupus-erythematosus-correlation-with-clinical-and-laboratory-parameters-of-disease-activity/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/does-erythrocyte-sedimentation-rate-reflect-and-discriminate-flare-from-infection-in-systemic-lupus-erythematosus-correlation-with-clinical-and-laboratory-parameters-of-disease-activity/