Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Radiographic axial spondyloarthritis (r-axSpA; formerly ankylosing spondylitis) has an average diagnostic delay of 7 years, which can lead to a diminished quality of life and disability if not promptly diagnosed and treated. While the impact of sex or gender on time to diagnosis has received considerable attention, the role of social determinants of health contributing to this delay remains understudied. We assessed whether time from the initial clinical documentation of r-axSpA symptoms to r-axSpA diagnosis varies based on sex, race, ethnicity, or the presence of social need.
Methods: We studied patients with r-axSpA using electronic health records from Boston Medical Center from 2000 to 2022. The cohort was built with the Observational Health Data Sciences and Informatics (OHDSI) network. We included adults with r-axSpA defined as 1 or more ICD-9 or 10 codes for r-axSpA who had outpatient visit information for > 12 months prior to r-axSpA diagnosis. For the primary analysis, we assessed the time from back pain/spinal pain to r-axSpA diagnosis and secondarily, the time to r-axSpA from either back/spine pain, peripheral arthritis, psoriasis, inflammatory bowel disease or uveitis. We extracted data on sex, patient-reported race, ethnicity, and documentation of any social need from an institutional validated questionnaire. We employed parametric survival models, accelerated failure time, to explore the average time to r-axSpA diagnosis, (1) from first diagnosis of back/spinal pain and (2) from any r-axSpA -related condition in the presence of unmet social needs.
Results: We included 404 patients with back pain or an r-axSpA -associated condition prior to r-axSpA diagnosis. Of these patients, 61 had at least one social need (mean age 49, 38.6 % female), with 25.5% of them identifying as Black and 31.1% as other or unknown race (Table). Patients with a documented social need had a 21% increase in time from back pain to r-axSpA diagnosis (95% CI 0.93, 1.56; Figure), adjusting for sex, race, and ethnicity. In the model for any r-axSpA -related condition, time to diagnosis increased similarly by 21% (95% CI 0.92, 1.57). Given that mean time to r-axSpA diagnosis was 34 months among those without social need, these findings indicate that a social need increased the time to r-axSpA diagnosis by 7 months, after accounting for age and sex.
Conclusion: This study reveals a trend toward diagnostic delay in r-axSpA related to social need, sex, race, and ethnicity. Future studies should focus on referral strategies to enable prompt diagnosis and optimize care.
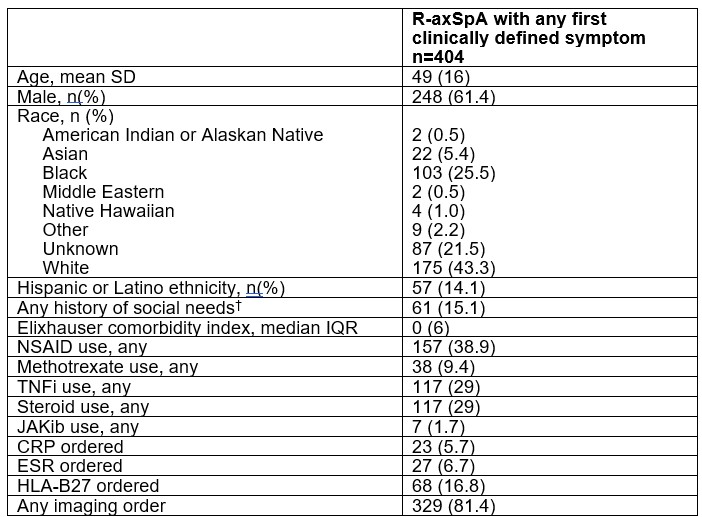
*Abbreviations: SD, standard deviation; IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drugs; TNFi, tumor necrosis factor inhibitor; JAKib, Janus kinase inhibitor; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; ED, emergency department
†Based on THRIVE questionnaire addressing categories of: housing stability, food security, transportation access, medication affordability, employment status, education status, and caregiver status.
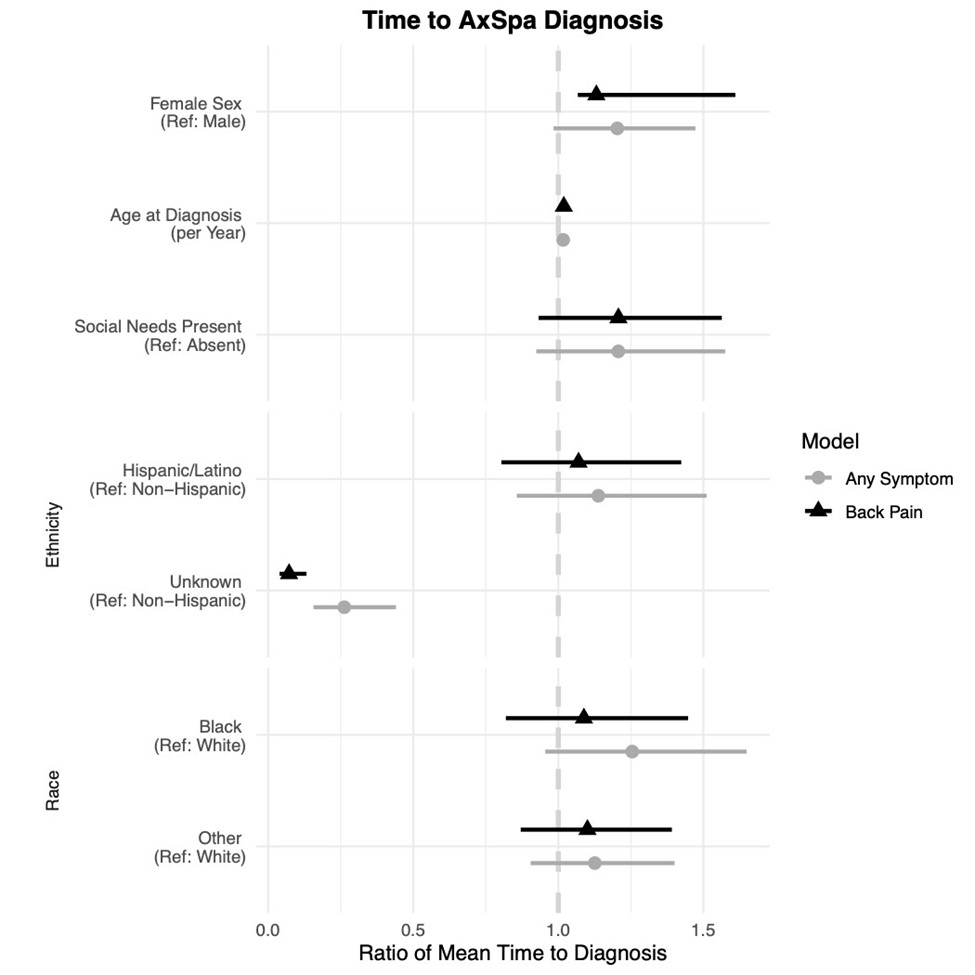
*The dotted line at 1 indicates that there is no difference in the average time it takes for the event to occur with an increase in the value of the risk factor. For example: those with social needs present have, on average, a 21% longer time to diagnosis compared to those without social needs, accounting for age, sex, race, and ethnicity.
To cite this abstract in AMA style:
Ferrandiz R, Rabasa G, Gasman S, Mcginley B, Stovall R, Jafarzadeh S, Liew J, Dubreuil M. Disparities in Time to Diagnosis for Radiographic Axial Spondyloarthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/disparities-in-time-to-diagnosis-for-radiographic-axial-spondyloarthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/disparities-in-time-to-diagnosis-for-radiographic-axial-spondyloarthritis/