Session Information
Date: Monday, October 27, 2025
Title: (1191–1220) Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Autoantibodies play a key role in the diagnosis, classification, and prognosis of idiopathic inflammatory myopathies (IIM). Among the most relevant are myositis-specific antibodies (MSAs), such as anti-Jo-1, and myositis-associated antibodies (MAAs), such as anti-Ro/Ro-52. Accurate serological detection using techniques such as Enzyme-Linked Immunosorbent Assay (ELISA) or immunoblot, is essential. However, in clinical practice, discordance between these methods is frequently observed. We aim to evaluate the discordance between ELISA and immunoblot in detecting Jo-1 and Ro/Ro-52 autoantibodies, and the clinical relevance of discordant results in a real-world cohort.
Methods: A retrospective, cross-sectional study was conducted on patients from a tertiary health center (Red de Salud UC Christus), who underwent testing for antinuclear antibodies (ANA), nuclear extractable antigen (ENA), and a myositis autoantibody panel within a +/-1 year interval, from March 2020 to March 2021 and had at least one clinic visit. ANA was detected using indirect immunofluorescence on HEp-2 cells, ENA by ELISA, and the myositis autoantibody panel by a 16-antigen line immunoassay/immunoblot. Demographic, clinical, and laboratory variables were collected through review of electronic medical records.
Results: A total of 112 patients met the inclusion criteria. 69 (61.6%) were female, with a mean age of 54.4 (±17.3) years. ANA was positive in 63 patients (53.4%), with the most frequent titer being 1/80 dilution, with AC-4,5 pattern (n=27, 23%). Jo-1 autoantibodies were detected exclusively by ELISA in 4 patients, exclusively by immunoblot in 5, and by both methods in 3. Ro/Ro-52 autoantibodies were positive exclusively by ELISA in 4 patients, exclusively by immunoblot in 14, and by both in 1. The discordance rate between ELISA and immunoblot was 8% for Jo-1 and 17% for Ro/Ro-52. Among the 3 patients with concordant Jo-1 positivity on both tests, all had dermatomyositis (DM)—two met definite and one met possible ACR/EULAR classification criteria. Of the 4 patients with positive Jo-1 on ELISA but negative on immunoblot, only one had DM; the remaining three had no autoimmune disease. In contrast, all patients who were Jo-1 negative on ELISA but positive on immunoblot had confirmed autoimmune conditions (Table 1). The one patient who had Ro positivity on ELISA and Ro-52 positivity on immunoblot was ultimately diagnosed with thyroid cancer. Finally, no correlation was observed between ANA patterns (nuclear or cytoplasmic) and specific autoantibodies identified by the other methods.
Conclusion: Our findings highlight a significant rate of discordance between ELISA and immunoblot in the detection of autoantibodies, particularly for Ro/Ro-52. Notably, immunoblot-identified Jo-1 positivity alone was more consistently associated with confirmed autoimmune diagnoses than ELISA alone. These results underscore the importance of using complementary serological methods in the diagnostic workup of suspected IIM, and caution against relying solely on a single testing modality.
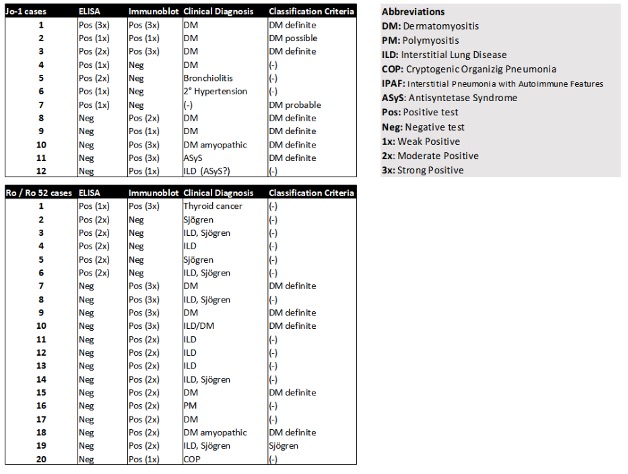 Clinical diagnoses and classification criteria according to Jo-1 and Ro/Ro-52 antibody result concordance and discordance between ELISA and immunoblot.
Clinical diagnoses and classification criteria according to Jo-1 and Ro/Ro-52 antibody result concordance and discordance between ELISA and immunoblot.
To cite this abstract in AMA style:
Valenzuela A, Cerda Acevedo S, Vera Gutiérrez F. Discordance between Immunoblot and ELISA in the detection of Jo-1 and Ro/Ro-52 Autoantibodies [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/discordance-between-immunoblot-and-elisa-in-the-detection-of-jo-1-and-ro-ro-52-autoantibodies/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/discordance-between-immunoblot-and-elisa-in-the-detection-of-jo-1-and-ro-ro-52-autoantibodies/